the Creative Commons Attribution 4.0 License.
the Creative Commons Attribution 4.0 License.
 | 22 Jun 2026
| 22 Jun 2026
Neutrophil extracellular trap (NET)-related index as an indicator of periprosthetic joint infection
Tingrun Cui
Yongjian Liang
Zeyu Feng
Libo Hao
Guoqiang Zhang
Ming Ni
Jing Sheng
Dihua Shangguan
Jiying Chen
Jun Fu
Background: Periprosthetic joint infection (PJI) is a devastating complication of arthroplasty and is difficult to diagnose accurately. This study aims to explore the value of neutrophil extracellular traps in synovial fluid (SF-NETs, web-like structures released by neutrophils as a critical innate immune response) for diagnosing PJI. Methods: A retrospective cohort study was conducted, enrolling post-arthroplasty subjects from January 2018 to December 2023. Three components of SF-NETs (cell-free double-strand DNA, SF-dsDNA; citrullinated histone H3, SF-CitH3; SF-Nucleosome) and SF-NETs1+ (positive with one out of the three NET components), SF-NETs2+ (positive with two out of the three NET components), white blood cell count (SF-WBC), polymorphonuclear cell percentage (SF-PMN %), neutrophil count in SF (SF-PMN), microbiological examinations (Culture) and infection-related systemic indices were evaluated. Results: A total of 64 of 153 included subjects were diagnosed as PJI. SF-dsDNA and SF-CitH3 had significantly higher levels in the PJI group compared to the non-PJI group (P < 0.001) and showed positive correlations with SF-WBC, SF-PMN % and SF-PMN (0.4 < ρ < 0.7), while SF-Nucleosome had no significant difference. Sensitivity and specificity of SF-NETs1+, SF-NETs2+ and Culture were 82.2 % and 78.7 %, 59.4 % and 95.5 %, and 54.1 % and 86.8 %, respectively. The NET related index (NETRI) was defined as 10.529 × SF-NETs 28.114 × SF-PMN % + 8.210 × Culture-1.452, with the area under the receiver operating characteristic curve of 0.922, making it a novel indicator. Conclusions: SF-NETs1+ and SF-NETs2+ may serve respectively in the screening and exclusion of PJI. NETRI represented a new discriminator for PJI diagnosis.
- Article
(1466 KB) - Full-text XML
- BibTeX
- EndNote




Periprosthetic joint infection (PJI) refers to infection around the joint prosthesis after implantation. Its incidence is about 2 %–4 % and has risen in recent years (Parvizi et al., 2011; Cai et al., 2023). PJI is an unexpected postoperative infection, distinct from primary or latent infections; despite the implementation of multiple evidence-based preventive strategies, PJI cannot be entirely eliminated (Parvizi et al., 2018). Delayed diagnosis and inadequate treatment can cause severe outcomes, prolonged hospitalization, delayed recovery, and heavy psychological and economic burdens (Rao et al., 2011; Parvizi et al., 2018).
Various laboratory markers have been studied for PJI diagnosis, including C-reactive protein (CRP), D-dimer, erythrocyte sedimentation rate (ESR), and synovial fluid (SF) white blood cell (WBC) count (SF-WBC), SF polymorphonuclear cell percentage (SF-PMN %), leukocyte esterase, and microbiological tests, as recommended by guidelines. However, diagnostic uncertainty persists (e.g., “possibly infected” or “infected likely”), and novel markers or techniques have continued to be explored, although many faced practical limitations (McNally et al., 2021; Parvizi and Gehrke, 2014; Parvizi et al., 2018; Sigmund et al., 2022).
Neutrophils are the most abundant effector cells in the innate immune system and play a central role in PJI pathogenesis. Neutrophil-related indices, such as α-defensin, CD-64 and neutrophil extracellular traps (NETs), have attracted attention. While α-defensin is a well-established diagnostic marker and CD64 shows good diagnostic potential, both are limited by time-consuming, costly and clinically inconvenient detection methods (Qin et al., 2020; Yuan et al., 2017). NETs consist of decondensed chromatin (mainly cell-free dsDNA), histones and nucleosomes (consisting exactly of nuclear dsDNA and histones) (Cutter and Hayes, 2015), forming large extracellular structures that trap and kill pathogens (Papayannopoulos, 2018). Recent studies have investigated NET components in synovial fluid (SF) for PJI diagnosis. Lögters et al. (2009) and Cobra et al. (2022) found significant differences in cell-free dsDNA between infection and non-infection groups. Cai et al. (2023) reported an area under the receiver operating characteristic (ROC) curve (AUC) of 0.971 for SF-NETs in 74 cases using a single enzyme-linked immunosorbent assay (ELISA) kit. De Sandes Kimura et al. (2024) showed AUCs of 0.94–1.00 for isolated NET constituents in 32 cases. However, prior studies had relatively small sample sizes and a high risk of bias, leaving changes in individual NET components unclear. We therefore conducted this retrospective cohort study to evaluate the diagnostic value of SF-NET constituents and their combinations for PJI diagnosis.
2.1 Subjects and specimens
This retrospective cohort study was conducted in patients with suspected PJI. From January 2018 to December 2023, 172 patients aged 18 years or older with suspected PJI after total joint arthroplasty and who underwent diagnostic laboratory testing were consecutively enrolled in the First Medical Center of Chinese PLA General Hospital. Exclusion criteria were cancer, liver cirrhosis, severe renal insufficiency and the absence of confirmed infection-related diagnoses or necessary data. The diagnosis of PJI was made following the Musculoskeletal Infection Society definition of PJI in 2014 (Parvizi and Gehrke, 2014) integrating all available data under the clinical scenario. This study was approved by the Ethics Committee of Chinese PLA General Hospital. We conducted the study following the principles of the Declaration of Helsinki and current ethics standards. All patients signed the written informed consent.
SF specimens from the included subjects were harvested via aseptic arthrocentesis, which were aliquoted and stored at −80 °C within 2 h of acquisition. Before storage, routine laboratory tests and pathogen cultures of SF were conducted. When conditions of “punctio sicca” were encountered, joint irrigations with sterile normal saline followed by aspirations of the lavage fluid were performed for microbiological analyses, and cytological studies were thus omitted due to dilution. At the same time, venous blood was collected into three tubes, containing 3.2 % sodium citrate, ethylene diamine tetra-acetic acid (EDTA) and clot activator (BD Biosciences, New Jersey, USA), respectively. Citrated whole blood was centrifuged at 1500 g at room temperature for 15 min to obtain the plasm. Clotted whole blood was centrifuged at 1500 g at room temperature for 15 min to obtain the serum.
2.2 Laboratory parameters
WBC count, neutrophil percentage (NEUT %) and platelet (PLT) count in EDTA-anticoagulated whole blood, as well as SF-WBC and SF-PMN %, were determined using a Sysmex XN-20 analyzer (Sysmex, Kobe, Japan). The absolute counts of neutrophils (NEUT) were calculated by multiplying the WBC and NEUT %, and the SF polymorphonuclear cell count (SF-PMN) was calculated as the product of SF-WBC and SF-PMN %. The levels of ESR and CRP in EDTA-anticoagulated whole blood were measured using a Greiner Bio-One SRS 100/II analyzer (Greiner Bio-One, Frickenhausen, Germany) and a Lifotronic PA-990 analyzer (Lifotronic, Shenzhen, China), respectively. The D-dimer level in plasma was measured using a Stago STA R Max analyzer (Stago, Paris, France). The interleukin-6 (IL-6) level in serum was measured using an Immulite 1000 immunoassay system (Siemens, Forchheim, Germany). For pathogen culture, the SF specimens were injected into BACT/ALERT PF Pediatric FAN vials and BACT/ALERT PF FA FAN vials, respectively, and detected using a BioMérieux BACT/ALERT system (BioMérieux, Marcy l'Etoile, France). All specimens for microbiological tests were incubated for up to 14 d unless the positive growth of pathogens, and the results, were documented as “Culture”.
2.3 Measurement of SF-NET components
The concentrations of the three main constituents of NETs in SF, including cell-free dsDNA (SF-dsDNA), citrullinated histone H3 (SF-CitH3) and nucleosomes (SF-Nucleosome), were measured (Liu et al., 2021). The SF aliquots were diluted twice with phosphate buffer solution. The kits were read using a SpectraMax M2 microplate reader (Molecular Devices, California, USA).
The Quant-iT™ PicoGreen® dsDNA Assay Kit (Invitrogen, California, USA) was applied to determine the concentration of SF-dsDNA. Two 96-well black plates (Corning, New York, USA) were utilized for fluorescence acquisition, with an excitation wavelength of 480 nm and an emission wavelength of 520 nm. The Citrullinate Histone H3 ELISA Kit (Cayman, Michigan, USA) was employed to measure SF-CitH3, with the absorption wavelength set at 450 nm. The SF-Nucleosome was measured using the Cell Death Detection ELISAPLUS Kit (Roche, Basel, Switzerland), and the value of absorption at the wavelength of 405 nm subtracted from that of 490 nm was adopted. The absorbance value of the negative control well was subtracted from that of the test well and the positive control well, respectively. Subsequently, the ratio of the resulting value for SF-Nucleosome concentration was calculated.
2.4 Statistical analysis
An IBM SPSS 26.0.0 (New York, USA) and GraphPad Prism 8.0.2 (Massachusetts, USA) were employed for statistical analysis. All data had non-normal distributions; thus, they were presented as median (25th, 75th percentiles). A Mann–Whitney U test was used to identify variables with statistically significant differences between the PJI and non-PJI groups. Spearman's rank correlation coefficient ρ was used for nonparametric correlation analysis. Outliers twice the interquartile range and larger than the 75th percentile were excluded in the linear regression analysis. Binomial logistic regression analysis was used to generate odds ratios (ORs), with 95 % confidence intervals (CI). An ROC curve analysis was adopted to estimate the diagnostic efficacy of the respective indices. All box plots were presented with the horizontal bars representing medians and the vertical bars representing the 2.5th and the 97.5th percentiles. P < 0.050 was considered as statistically significant.
3.1 Demographic and clinical characteristics of subjects
Of the total of 172 subjects, 19 fulfilled the exclusion criteria, and the rest were included in the study. Among the 153 subjects, 64 were diagnosed with PJI, all of which were classified as chronic PJI based on the available medical history and diagnostic findings. The demographic and clinical characteristics of the two groups are shown in Table 1. The median age of participants was 67.0 (60.0, 72.0) years, with a significant difference between the PJI and non-PJI groups (P=0.021). There were 41 hips and 112 knees involved in total, with no significant difference between groups (P=0.494).
The results for all parameters in the two groups are displayed in Table 2. We found that PJI patients had higher levels of SF-dsDNA and SF-CitH3 than non-PJI patients (P < 0.001 for both), but there is no significant difference in SF-Nucleosome (P=0.135).
Table 1Demographic and clinical characteristics of infected and non-infected patientsa.

a Data proven to be non-normally distributed are showed as median (25th, 75th percentiles). b P < 0.050, and the difference is statistically significant when compared with patients with PJI. Abbreviations: PJI, periprosthetic joint infection.
Table 2Parameters in infected and non-infected patientsa.
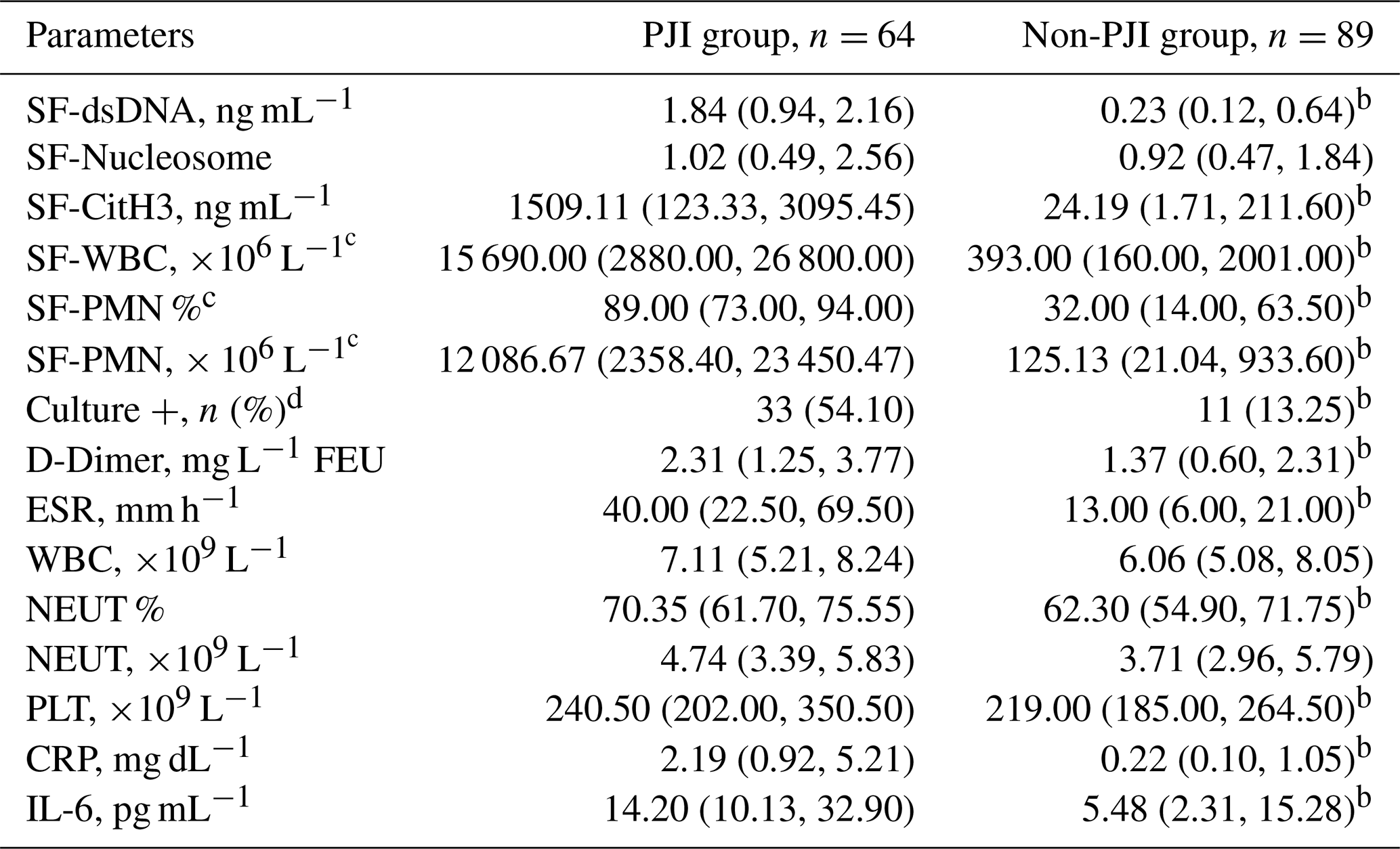
a Data proven to be non-normally distributed are showed as median (25th, 75th percentiles). b P < 0.050, and the difference is statistically significant when compared with patients with PJI. c Levels of SF-PMN(%) and SF-WBC were examined on SF of 45 randomly selected from 64 PJI patients and 47 from 89 non-PJI patients. d Culture were evaluated on SF of 61 randomly selected from 64 PJI patients and 83 from 89 non-PJI patients. Abbreviations: PJI, periprosthetic joint infection; SF, synovial fluid; SF-dsDNA, double-stranded DNA in synovial fluid; SF-Nucleosome, nucleosome in synovial fluid; SF-CitH3, citrullinated histone H3 in synovial fluid; SF-WBC, white blood cell in synovial fluid; SF-PMN %, polymorphonuclear cell percentage in synovial fluid; SF-PMN, polymorphonuclear cell count in synovial fluid; ESR, erythrocyte sedimentation rate; WBC, white blood cell; NEUT %, neutrophil percentage; NEUT, neutrophil; PLT, platelet; CRP, C-reactive protein; IL-6, interleukin-6.
Notably, the SF-WBC level in PJI group was almost 40 times higher than that in non-PJI group (P < 0.001). Compared to the patients without PJI, the levels of SF-PMN % and SF-PMN were higher in those with PJI (P < 0.001 for both). For Culture, the number of positive cases in the PJI group was significantly more than that of non-PJI group (P < 0.001); and the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were 54.10 %, 86.75 %, 75.00 % and 72.00 %, respectively. Among the 33 Culture-positive subjects in the PJI group, staphylococci were the predominant pathogens, with Staphylococcus aureus isolated in eight cases (24 %) and coagulase-negative staphylococci (CoNS) in nine cases (27 %; S. epidermidis, S. haemolyticus, S. hominis, S. warneri, S. caprae and S. lugdunensis). Other organisms included enterococci (four cases), Gram-negative bacilli (four cases), viridans group streptococci and S. agalactiae (two cases), Candida parapsilosis (two cases), Brucella spp. (two cases), and occasional Micrococcus and rapidly growing mycobacteria. Three polymicrobial cases were identified. Among the non-PJI cases, 11 had a single positive Culture result, including five CoNS, two Gram-negative bacilli, two Bacillus spp. and two Rhizopus spp.
There is no significant difference in the level of WBC between two groups (P=0.293). However, compared to non-PJI patients, the level of NEUT % was higher in PJI patients (P=0.002), and the level of NEUT tended to be higher in patients with PJI (P=0.053). Patients without PJI manifested lower levels of D-dimer than those with PJI (P=0.008). Compared to the non-PJI group, the levels of ESR and PLT were higher in patients with PJI (P < 0.001 and P=0.020, respectively). Finally, the levels of CRP and IL-6 demonstrated a significant increase in the PJI group compared to the non-PJI group (P < 0.001 for both).
3.2 Correlation between SF-NET components and WBC-related indices in SF
A correlation analysis was conducted between NET constituents (SF-dsDNA, SF-Nucleosome and SF-CitH3) and SF-WBC, SF-PMN % and SF-PMN. As shown in Fig. 1, there were positive correlations between SF-dsDNA and SF-WBC (ρ=0.464, P < 0.001), SF-PMN % (ρ=0.455, P < 0.001) and SF-PMN (ρ=0.535, P < 0.001). Similarly, SF-CitH3 also showed significant positive correlations with SF-WBC (ρ=0.436, P < 0.001), SF-PMN % (ρ=0.446, P < 0.001) and SF-PMN (ρ=0.494, P < 0.001) (Fig. 1). SF-Nucleosome was not significantly correlated with local WBC-related indices (P>0.050).
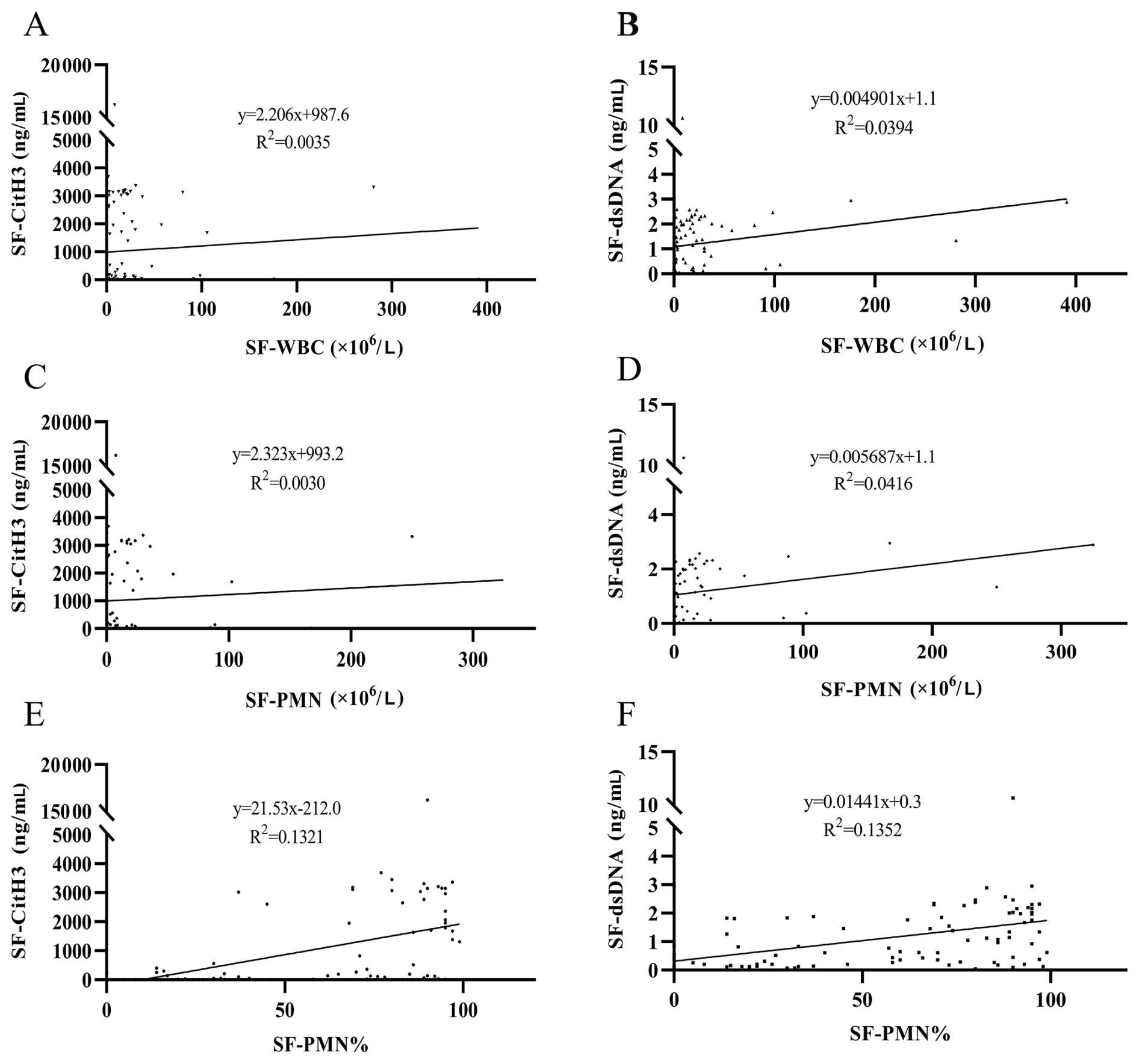
Figure 1Correlation analysis of SF-CitH3 and SF-dsDNA with SF-WBC, SF-PMN and SF-PMN %, respectively. (A) Correlation analysis between SF-CitH3 and SF-WBC. (B) Correlation analysis between SF-dsDNA and SF-WBC. (C) Correlation analysis between SF-CitH3 and SF-PMN. (D) Correlation analysis between SF-dsDNA and SF-PMN. (E) Correlation analysis between SF-CitH3 and SF-PMN %. (F) Correlation analysis between SF-dsDNA and SF-PMN %. Abbreviations: SF-dsDNA, double-stranded DNA in synovial fluid; SF-CitH3, citrullinated histone H3 in synovial fluid; SF-WBC, white blood cell in synovial fluid; SF-PMN %, polymorphonuclear cell percentage in synovial fluid; SF-PMN, polymorphonuclear cell count in synovial fluid.
3.3 Diagnostic efficacy evaluation for the identified indicators
ROC analyses were performed for all three components of SF-NETs, as well as for all indices that differed significantly between the PJI and non-PJI groups, including SF-WBC, SF-PMN %, SF-PMN, D-dimer, ESR, NEUT %, PLT, CRP and IL-6. The ROC curves of the different indicators are depicted in Fig. 2. As shown in Table 3, the AUC values of SF-dsDNA (0.844) and SF-CitH3 (0.821) were both greater than 0.800, and the AUC values of SF-PMN % (0.847) and SF-PMN (0.842) were similar to the AUC value of SF-dsDNA. The AUC values of SF-Nucleosome, SF-WBC, D-dimer, ESR, NEUT %, PLT, CRP and IL-6 were 0.571, 0.808, 0.637, 0.781, 0.649, 0.614, 0.798 and 0.721, respectively. The cutoff values of these indicators were calculated by the Youden index as 1.038 ng mL−1 (SF-dsDNA), 2.050 (SF-Nucleosome), 1171.694 ng mL−1 (SF-CitH3), 2095.000 × 106 L−1 (SF-WBC), 68.500 % (SF-PMN %), 947.800 × 106 L−1 (SF-PMN), 1.195 mg L−1 FEU (D-dimer), 18.500 mm h−1 (ESR), 66.900 % (NEUT %), 267.000 × 109 L−1 (PLT), 1.235 mg dL−1 (CRP) and 8.915 pg mL−1 (IL-6). The sensitivity, specificity, PPV and NPV of the identified factors were calculated using their cutoff values, and SF-CitH3 displayed the highest specificity (95.5 %) (Table 3).
Table 3Diagnostic values of the identified indicators.
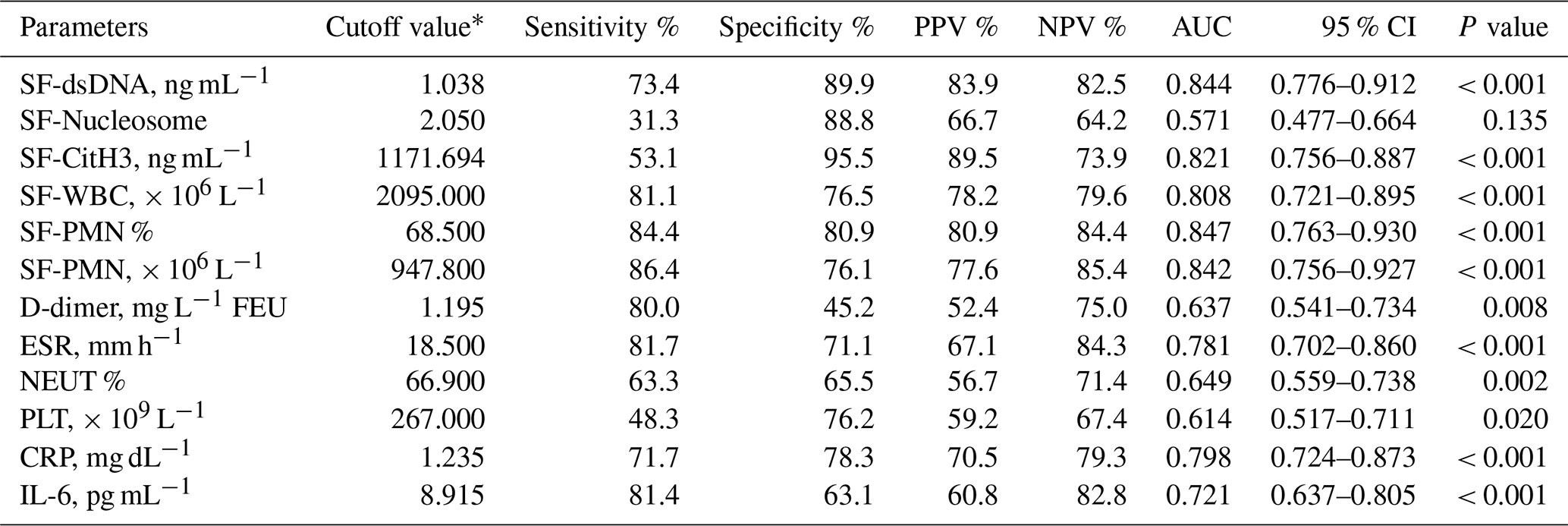
∗ All cutoff values were determined by the Youden index. Abbreviations: SF, synovial fluid; SF-dsDNA, double-stranded DNA in synovial fluid; SF-Nucleosome, nucleosome in synovial fluid; SF-CitH3, citrullinated histone H3 in synovial fluid; SF-WBC, white blood cell count in synovial fluid; SF-PMN %, polymorphonuclear cell percentage in synovial fluid; SF-PMN, polymorphonuclear cell count in synovial fluid; ESR, erythrocyte sedimentation rate; NEUT %, neutrophil percentage; PLT, platelet; CRP, C-reactive protein; IL-6, interleukin-6; PPV, positive predictive value; NPV, negative predictive value; AUC, area under the curve; CI, confidence interval.
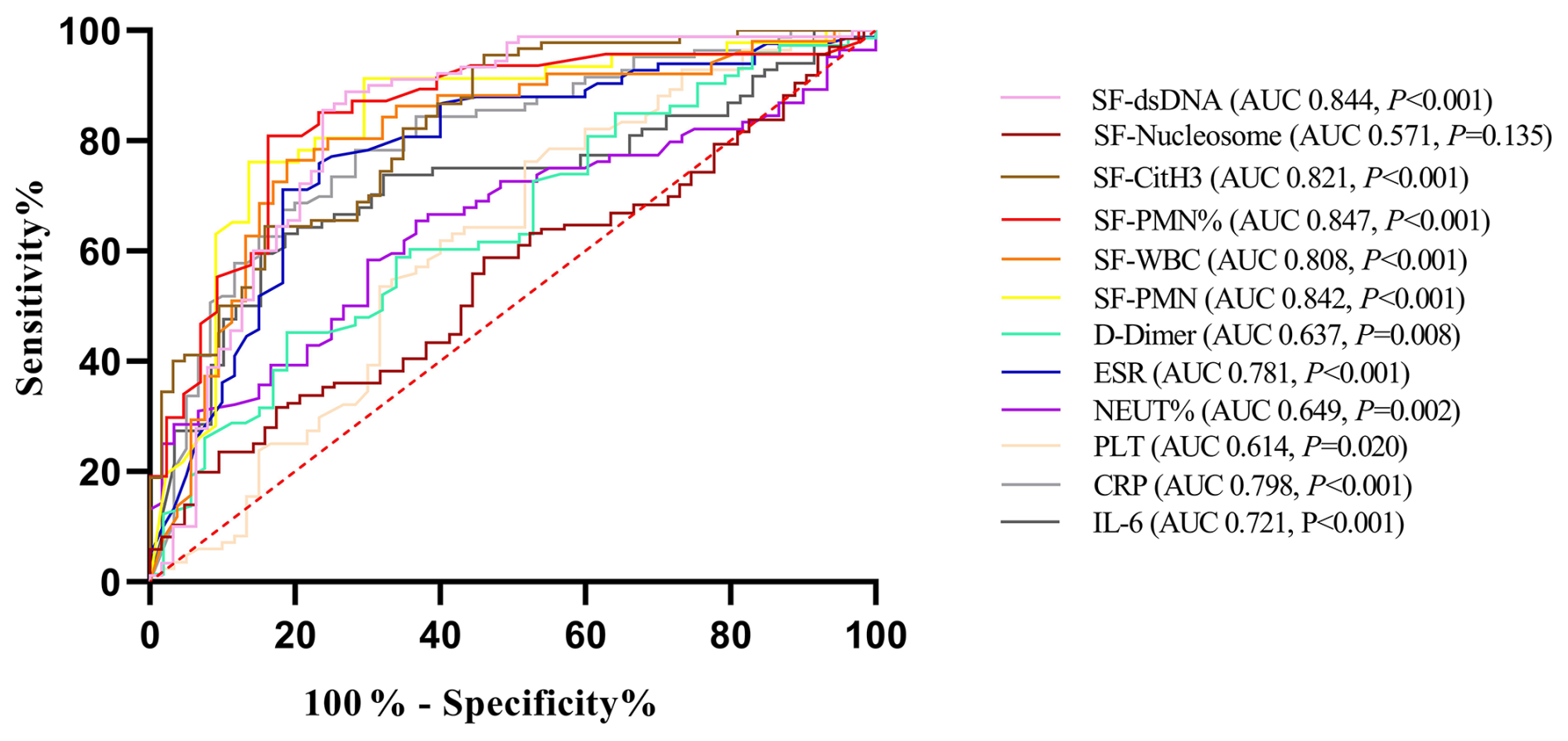
Figure 2Receiver operating characteristic curve analysis of the identified indicators for periprosthetic joint infection. Abbreviations: SF, synovial fluid; SF-dsDNA, double-stranded DNA in synovial fluid; SF-Nucleosome, nucleosome in synovial fluid; SF-CitH3, citrullinated histone H3 in synovial fluid; SF-PMN %, polymorphonuclear cell percentage in synovial fluid; SF-WBC, white blood cell in synovial fluid; SF-PMN, polymorphonuclear cell count in synovial fluid; ESR, erythrocyte sedimentation rate; NEUT %, neutrophil percentage; PLT, platelet; CRP, C-reactive protein; IL-6, interleukin-6.
3.4 The performance of SF-NET components
To further analyze the diagnostic value of SF-NETs for PJI, different combinations were identified. For instance, according to the ROC curve analysis, SF-NETs2+ was categorized when the test values of two out of the three components were equal to or greater than their respective cutoff values. Similarly, SF-NETs1+ and SF-NETs3+ were also documented (Table 4). As shown in Table 4, SF-NETs1+ displayed the greatest sensitivity (82.8 %), and the sensitivity of SF-NETs2+ and SF-NETs3+ were 59.4 % and 15.6 %, respectively. Meanwhile, SF-NETs3+ exhibited the largest specificity of 100.0 %, and the specificity of SF-NETs1+ and SF-NETs2+ were 78.7 % and 95.5 %, respectively. Additionally, among the NETs1+ false-negative subjects, four cases yielded positive cultures, comprising three cases of CoNS and one case of enterococci.
Table 4Combinations of NET components for PJI recognition∗.

∗ Subjects with one, two and three out of three components of NETs being positive were marked as NETs1+, NETs2+ and NETs3+, respectively. Abbreviations: PJI, periprosthetic joint infection; NETs, neutrophil extracellular traps.
3.5 Sifting of risk factors for PJI
A binomial logistic regression analysis was conducted to identify the risk factors of PJI. Variables that were independently and significantly different between the PJI and non-PJI groups – including age, SF-NETs1+, SF-PMN %, SF-WBC, Culture, D-dimer, ESR, NEUT %, WBC, PLT, CRP, and IL-6, were included into the analysis. Three indices, namely SF-NETs1+, SF-PMN % and Culture – were independent risk factors for PJI (Table 5). A larger number of SF-NETs1+ (P=0.001) and Culture (P=0.010) were associated with the increased risk of PJI. Furthermore, high levels of SF-PMN % (P=0.003) increased the risk of PJI.
Table 5Independent risk factors for PJI.
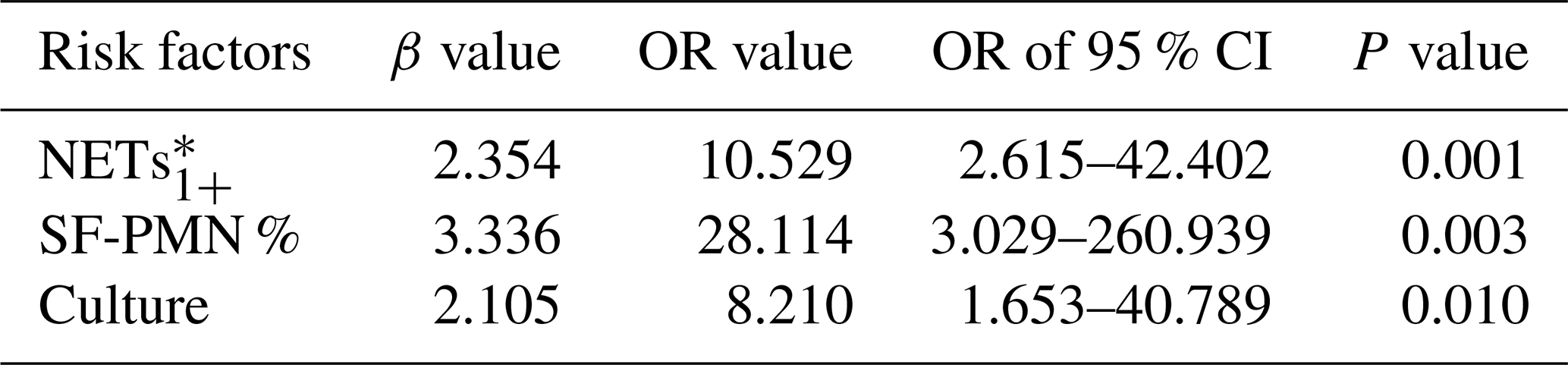
∗ Subjects with one out of three components of NETs being positive were marked as NETs1+. Abbreviations: PJI, periprosthetic joint infection; NETs, neutrophil extracellular traps; SF-PMN %, polymorphonuclear cell percentage in synovial fluid fibrinogen; CI, confidence interval; OR, odds ratio.
Consequently, a formula was developed to calculate a new indicator named NET related index (NETRI): NETRI = 10.529 × SF-NETs × SF-PMN % + 8.210 × Culture − 1.452. In this formula, the positive results of SF-NETs1+ and Culture were marked as “1” and their negative results were marked as “0”. As shown in Fig. 3A, compared to patients without PJI, patients with PJI exhibited significantly higher levels of NETRI [0.483 (−0.751, 1.376) vs. 4.138 (3.571, 6.009), P < 0.001]. The ROC curve analysis was conducted for NETRI (Fig. 3B), yielding an AUC of 0.922 (95 % CI: 0.862–0.981) with a cutoff value of 3.346. The sensitivity, specificity, PPV and NPV of NETRI were 82.2 %, 93.6 %, 92.5 % and 84.6 %, respectively.
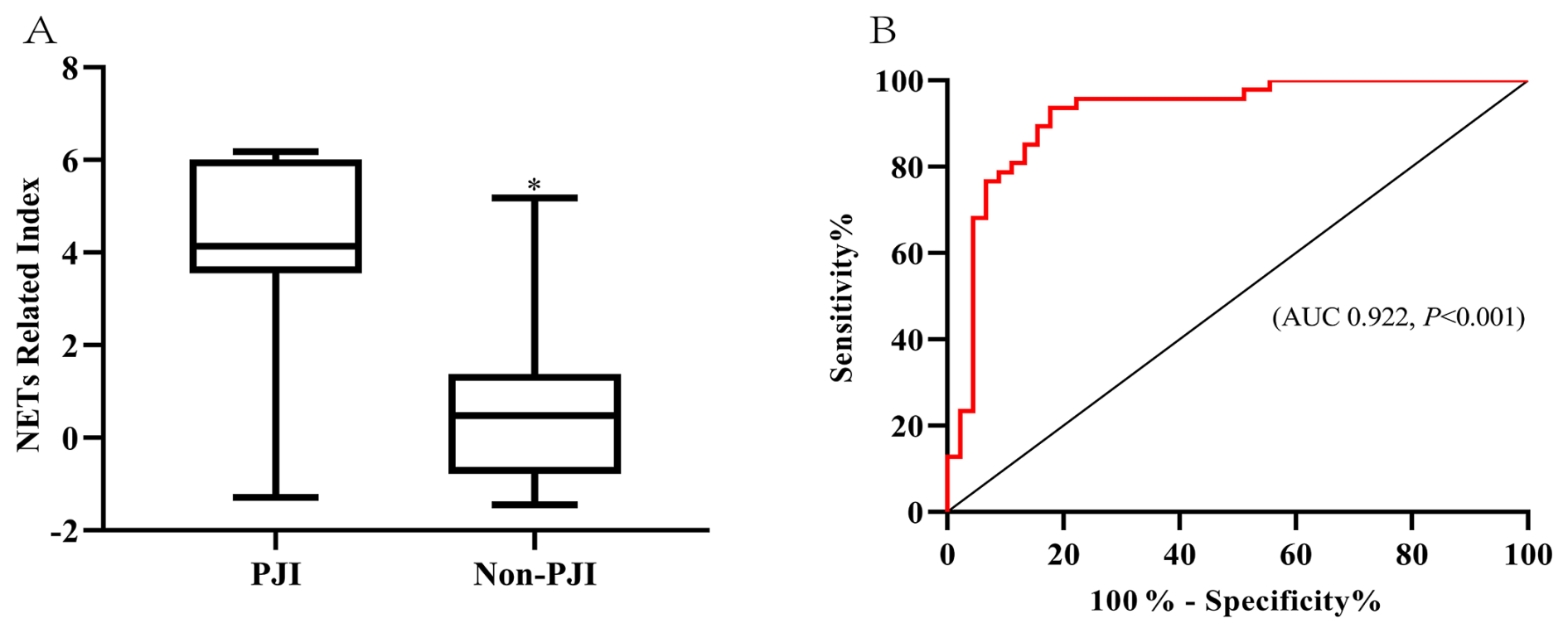
Figure 3The diagnostic value of NET related index for periprosthetic joint infection. (A) Comparison of the NET related index between patients with or without PJI. * P < 0.050, and the difference is statistically significant. For the box plots shown, the horizontal bars represent medians and the vertical bars show the 2.5th and 97.5th percentiles. (B) Receiver operating characteristic curve analysis of NET related index for periprosthetic joint infection. Abbreviations: PJI, periprosthetic joint infection; NET, neutrophil extracellular traps.
PJI, a severe complication of arthroplasty, has increased in incidence recently. Despite efforts, integrating traditional and novel markers for accurate PJI diagnosis remains challenging (Parvizi et al., 2018). Neutrophils dominate in PJI and release NETs through NETosis. NETs indicate neutrophil activation and may aid PJI diagnosis (Papayannopoulos, 2018). While NETs show value in systemic infections (Kumar et al., 2019), few studies address their role in PJI, and prior works measured NETs incompletely or with small samples (Cai et al., 2023; Lögters et al., 2009; Cobra et al., 2022; de Sandes Kimura et al., 2024). This study, with a larger cohort, measured SF-dsDNA, SF-CitH3 and SF-Nucleosome as NET components. Significant differences were observed in SF-dsDNA and SF-CitH3, but not in SF-Nucleosome, between PJI and non-PJI groups. SF-Nucleosome degradation into dsDNA and histones may explain this (Cutter and Hayes, 2015). Subsequently, we analyzed different numbers of NET components. SF-NETs1+ demonstrated higher sensitivity (82.8 %), while SF-NETs2+ exhibited higher specificity (95.5 %) with acceptable sensitivity (59.4 %). Given PJI's irreversible damage, sensitive screening with SF-NETs1+ suited initial visits; SF-NETs2+ better supports specific post-treatment confirmation. This tiered approach may prove useful.
Routine SF-WBC and SF-PMN % performed well for PJI diagnosis (Lee et al., 2017) and was further confirmed in our study, along with SF-PMN (all presented an AUC > 0.800). Therefore, aseptic arthrocentesis remains essential, with confirmed low iatrogenic infection risk (Keating et al., 2023), although such risk accumulates with repeated SF harvest. Furthermore, SF-dsDNA and SF-CitH3 positively correlated with local WBC indicators (0.4 < ρ < 0.7), consistent with NET origins (Dilley et al., 2023).
Pathogen culture, long the “gold standard” for PJI (Lagier et al., 2015), showed only 54.1 % sensitivity with 86.8 % specificity. Such high false negatives necessitated repeated sampling and limited practicability in drug sensitivity assessment and antibiotics selection (Bettencourt and Linder, 2010). There were four positive Culture results observed in NET1+ false-negative subjects. This may be attributable to prolonged disease duration, potential suboptimal joint fluid storage and random errors. However, the limited number of culture results and substantial missing data confer a high risk of bias, markedly limiting the reference value. Systemic markers (PLT, ESR, WBC, NEUT %, NEUT count, CRP, D-dimer, IL-6) showed limited diagnostic value (most AUC < 0.800), as circulatory indices poorly reflect local PJI, and were therefore adopted by clinical guidelines as combined markers or with weight points assigned (Sigmund et al., 2022).
Logistic regression identified SF-NETs1+, SF-PMN % and Culture as independent risk factors, which were all local indices. A new composite indicator, NETRI, achieved an AUC of 0.922, incorporating and outperforming all of these three markers. SF-NETs1+ was included due to its higher sensitivity, which was more suitable for uncertain PJI diagnosis. However, the current NET assay kits involved cumbersome procedures, and simplification of the kits is essential to meet clinical demands.
Indeed, determining the components of NETs separately was still quite complicated for clinical settings. Therefore, it is necessary to design an integrated assay kit for NETs and to conduct necessary validation. A meta-analysis indicated that SF-PMN % has a superior predictive value in PJI, with a sensitivity and specificity of 89 % and 86 % (Lee et al., 2017). Our study also confirmed SF-PMN % as another independent predictor for PJI. Additionally, as the “gold standard”, Culture was also included.
Patients with PJI in our study were 3 years older than those in the non-PJI group, and the median ages were both more than 65 years old. However, age was not identified in the present logistic regression analysis, which aligned with prior studies rejecting age as an independent risk factor (Inoue et al., 2019). While older age affected PJI primarily via other factors rather than independently, it remained noteworthy given the greater comorbidity complexity in elderly patients.
There are several limitations to this study. Our study was a single-center study, which may limit the generalizability of our findings, and future multi-center studies should be conducted. Then, due to missing data, pathogen data were simply described and were not analyzed in detail to avoid bias. Thus, our findings primarily apply to chronic PJI and suggest potential utility of NET-related markers; however, further subgroup analyses by pathogen virulence in larger cohorts are warranted to confirm generalizability, particularly for low-grade organisms. Additionally, the relatively small training set used for developing NETRI might have affected its diagnostic efficacy, and a larger sample size is necessary for validation.
Two out of the three components of SF-NETs, namely SF-dsDNA and SF-CitH3, were elevated in the PJI group compared to the non-PJI group. SF-dsDNA and SF-CitH3 showed significant positive correlations with local WBC status. SF-NETs1+ and SF-NETs2+ were proven to be suitable for PJI pre-treatment screening and post-treatment exclusion, respectively. Using binomial logistic analysis, a novel index named NETRI was developed based on SF-NETs1+, SF-PMN % and Culture, and can serve as a potential diagnostic indicator for PJI.
The data that support the findings of this study are available from the corresponding author upon reasonable request. The data cannot be made publicly available due to ethical concerns and privacy restrictions.
CTR, LYJ, CJY and FJ participated in the conception and design of the study. CTR, LYJ, FZY, HLB, ZGQ and NM participated in the literature search and data collection. SJ and SGDH provided assistance in the experimental measurement of the NET components. CTR, LYJ, CJY and FJ analyzed and interpreted the data. CTR and LYJ drafted the paper, which was critically reviewed by all authors. All authors subsequently approved the final article for submission.
The contact author has declared that none of the authors has any competing interests.
This study was approved by the Ethics Committee of Chinese PLA General Hospital (no. S2021-015-01). We conducted the study following the principles of the Declaration of Helsinki and current ethics standards. All patients signed the written informed consent.
Publisher's note: Copernicus Publications remains neutral with regard to jurisdictional claims made in the text, published maps, institutional affiliations, or any other geographical representation in this paper. The authors bear the ultimate responsibility for providing appropriate place names. Views expressed in the text are those of the authors and do not necessarily reflect the views of the publisher.
This research has been supported by the National Key Research and Development Program of China (grant no. 2023YFB4705600) and the Youth Project of National Natural Science Foundation of China (grant no. 82102585).
This paper was edited by Derek Amanatullah and reviewed by two anonymous referees.
Bettencourt, R. B. and Linder, M. M.: Arthrocentesis and Therapeutic Joint Injection: An Overview for the Primary Care Physician, Primary Care, 37, 691–702, https://doi.org/10.1016/j.pop.2010.07.002, 2010.
Cai, Y., Liang, J., Chen, X., Zhang, G., Jing, Z., Zhang, R., Lv, L., Zhang, W., and Dang, X.: Synovial fluid neutrophil extracellular traps could improve the diagnosis of periprosthetic joint infection, Bone Joint Res., 12, 113–120, https://doi.org/10.1302/2046-3758.122.Bjr-2022-0391.R1, 2023.
Cobra, H., Mozella, A. P., da Palma, I. M., Salim, R., and Leal, A. C.: Cell-free Deoxyribonucleic Acid: A Potential Biomarker of Chronic Periprosthetic Knee Joint Infection, J. Arthroplasty, 37, 2455–2459, https://doi.org/10.1016/j.arth.2022.07.002, 2022.
Cutter, A. R. and Hayes, J. J.: A brief review of nucleosome structure, FEBS Lett., 589, 2914–2922, https://doi.org/10.1016/j.febslet.2015.05.016, 2015.
de Sandes Kimura, O., Mozella, A., Cobra, H., Maciel Saraiva, A. C., Carvalho de Almendra Freitas, E. H., Cury Fernandes, M. B., Matheus Guimarães, J. A., Defino, H., and Leal, A. C.: Neutrophil Extracellular Trap-related Biomarkers Are Increased in the Synovial Fluid of Patients With Periprosthetic Joint Infections, Clin. Orthop. Relat. Res., 482, 727–733, https://doi.org/10.1097/corr.0000000000002891, 2024.
Dilley, J. E., Seetharam, A., Meneghini, R. M., and Kheir, M. M.: Synovial Fluid Absolute Neutrophil Count and Neutrophil-To-Lymphocyte Ratio are not Superior to Polymorphonuclear Percentage in Detecting Periprosthetic Joint Infection, J. Arthroplasty, 38, 146–151, https://doi.org/10.1016/j.arth.2022.07.005, 2023.
Inoue, D., Xu, C., Yazdi, H., and Parvizi, J.: Age alone is not a risk factor for periprosthetic joint infection, J. Hosp. Infect., 103, 64–68, https://doi.org/10.1016/j.jhin.2019.04.005, 2019.
Keating, T. C., Guntin, J., Harkin, W. E., Weintraub, M. T., Karas, V., and Berger, R. A.: Low Risk of Acute Iatrogenic Periprosthetic Joint Infection After Prosthetic Joint Aspiration, J. Arthroplasty, 38, 1861–1863, https://doi.org/10.1016/j.arth.2023.03.053, 2023.
Kumar, S., Gupta, E., Kaushik, S., Srivastava, V. K., Saxena, J., Mehta, S., and Jyoti, A.: Quantification of NETs formation in neutrophil and its correlation with the severity of sepsis and organ dysfunction, Clin. Chim. Acta, 495, 606–610, https://doi.org/10.1016/j.cca.2019.06.008, 2019.
Lagier, J. C., Edouard, S., Pagnier, I., Mediannikov, O., Drancourt, M., and Raoult, D.: Current and past strategies for bacterial culture in clinical microbiology, Clin. Microbiol. Rev., 28, 208–236, https://doi.org/10.1128/cmr.00110-14, 2015.
Lee, Y. S., Koo, K. H., Kim, H. J., Tian, S., Kim, T. Y., Maltenfort, M. G., and Chen, A. F.: Synovial Fluid Biomarkers for the Diagnosis of Periprosthetic Joint Infection: A Systematic Review and Meta-Analysis, J. Bone Joint Surg. Am., 99, 2077–2084, https://doi.org/10.2106/jbjs.17.00123, 2017.
Liu, L., Zhang, W., Su, Y., Chen, Y., Cao, X., and Wu, J.: The impact of neutrophil extracellular traps on deep venous thrombosis in patients with traumatic fractures, Clin. Chim. Acta, 519, 231–238, https://doi.org/10.1016/j.cca.2021.04.021, 2021.
Lögters, T., Paunel-Görgülü, A., Zilkens, C., Altrichter, J., Scholz, M., Thelen, S., Krauspe, R., Margraf, S., Jeri, T., Windolf, J., and Jäger, M.: Diagnostic accuracy of neutrophil-derived circulating free DNA (cf-DNA/NETs) for septic arthritis, J. Orthop. Res., 27, 1401–1407, https://doi.org/10.1002/jor.20911, 2009.
McNally, M., Sousa, R., Wouthuyzen-Bakker, M., Chen, A. F., Soriano, A., Vogely, H. C., Clauss, M., Higuera, C. A., and Trebše, R.: The EBJIS definition of periprosthetic joint infection, Bone Joint J., 103-b, 18–25, https://doi.org/10.1302/0301-620x.103b1.Bjj-2020-1381.R1, 2021.
Papayannopoulos, V.: Neutrophil extracellular traps in immunity and disease, Nat. Rev. Immunol., 18, 134–147, https://doi.org/10.1038/nri.2017.105, 2018.
Parvizi, J. and Gehrke, T.: Definition of periprosthetic joint infection, J. Arthroplasty, 29, 1331, https://doi.org/10.1016/j.arth.2014.03.009, 2014.
Parvizi, J., Jacovides, C., Zmistowski, B., and Jung, K. A.: Definition of periprosthetic joint infection: is there a consensus?, Clin. Orthop. Relat. Res., 469, 3022–3030, https://doi.org/10.1007/s11999-011-1971-2, 2011.
Parvizi, J., Tan, T. L., Goswami, K., Higuera, C., Della Valle, C., Chen, A. F., and Shohat, N.: The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria, J. Arthroplasty, 33, https://doi.org/10.1016/j.arth.2018.02.078, 2018.
Qin, L., Hu, N., Li, X., Chen, Y., Wang, J., and Huang, W.: Evaluation of synovial fluid neutrophil CD64 index as a screening biomarker of prosthetic joint infection, Bone Joint J, 102-B, 463–469, https://doi.org/10.1302/0301-620X.102B4.BJJ-2019-1271.R1, 2020.
Rao, N., Ziran, B. H., and Lipsky, B. A.: Treating osteomyelitis: antibiotics and surgery, Plast. Reconstr. Surg., 127, 177s–187s, https://doi.org/10.1097/PRS.0b013e3182001f0f, 2011.
Sigmund, I. K., Luger, M., Windhager, R., and McNally, M. A.: Diagnosing periprosthetic joint infections: a comparison of infection definitions: EBJIS 2021, ICM 2018, and IDSA 2013, Bone Joint Res., 11, 608–618, https://doi.org/10.1302/2046-3758.119.Bjr-2022-0078.R1, 2022.
Yuan, J., Yan, Y., Zhang, J., Wang, B., and Feng, J.: Diagnostic accuracy of alpha-defensin in periprosthetic joint infection: a systematic review and meta-analysis, Int. Orthop., 41, 2447–2455, https://doi.org/10.1007/s00264-017-3647-3, 2017.