| 05 Jan 2023
| 05 Jan 2023
Clinical–epidemiological profile of confirmed cases of osteoarticular tuberculosis
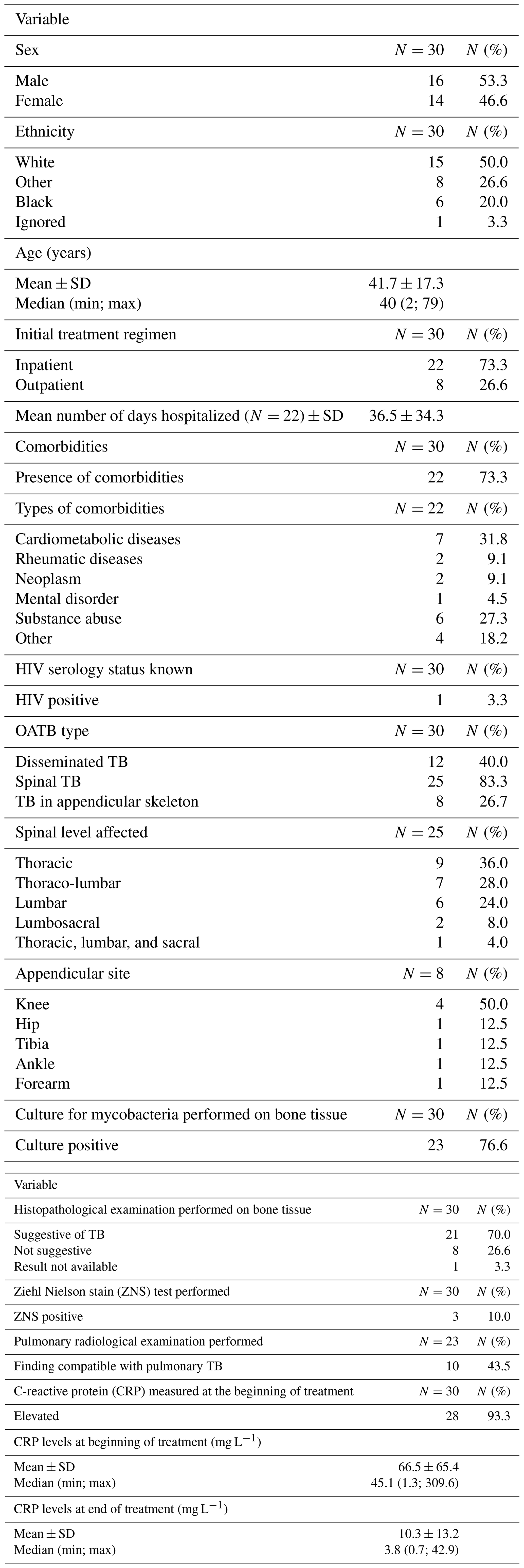
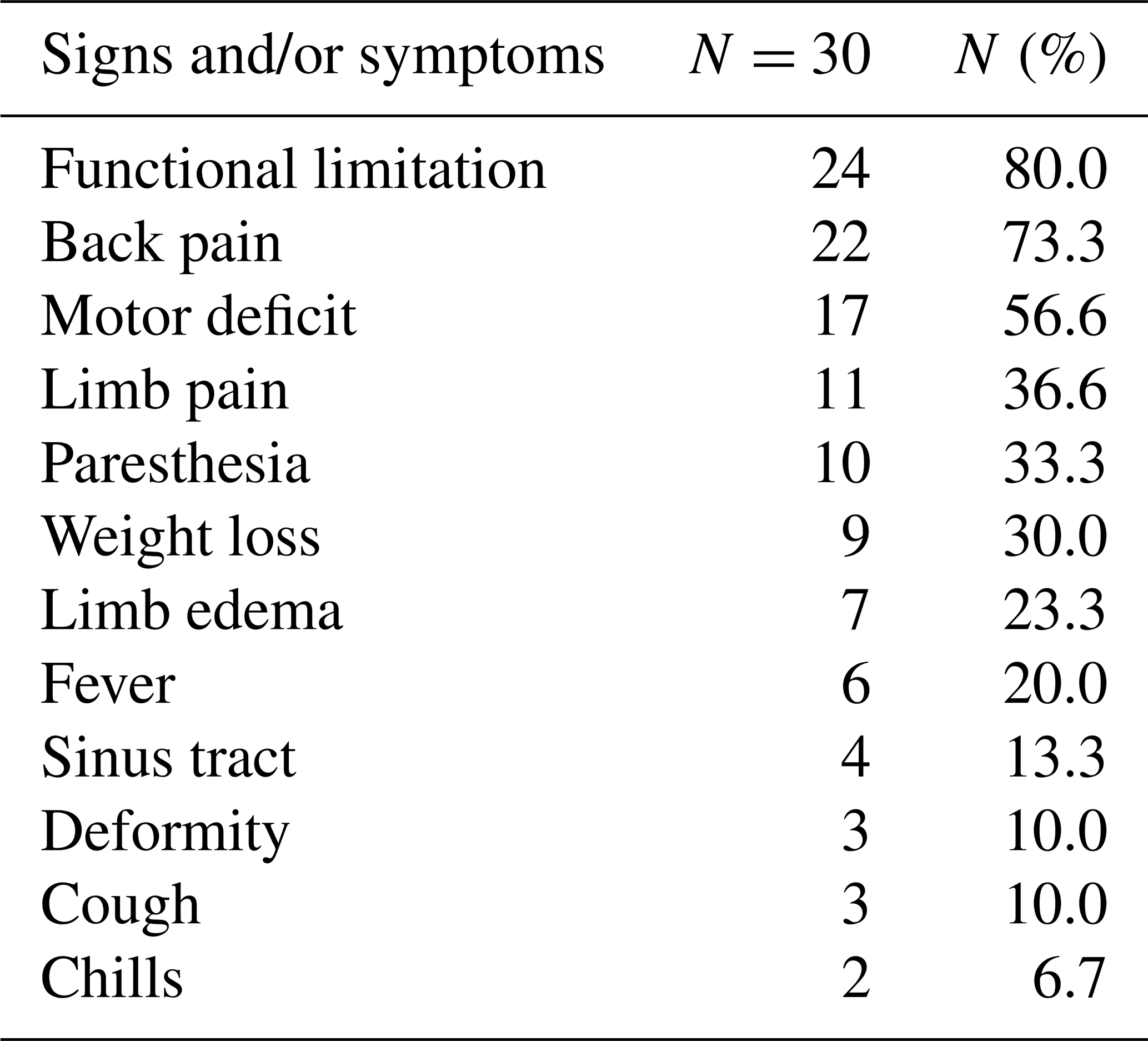
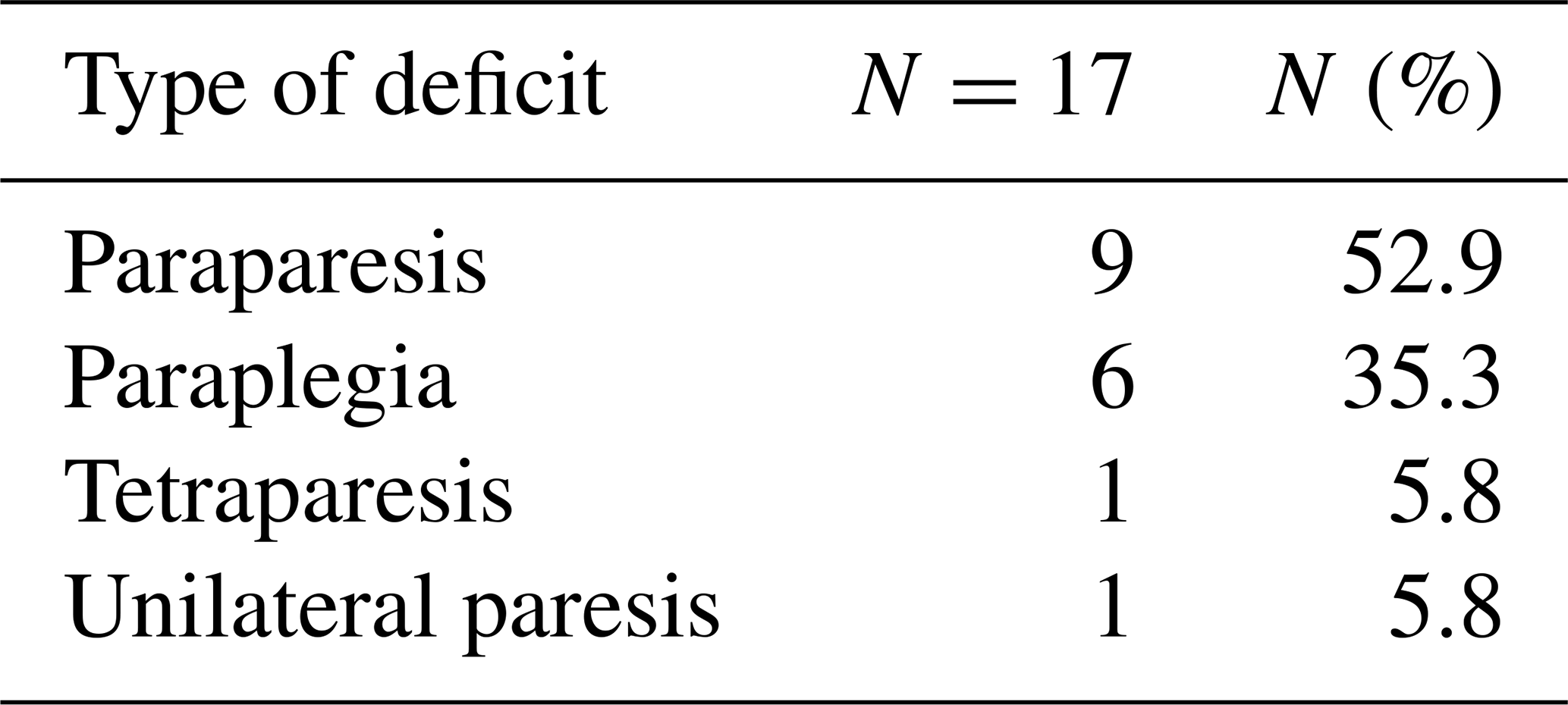
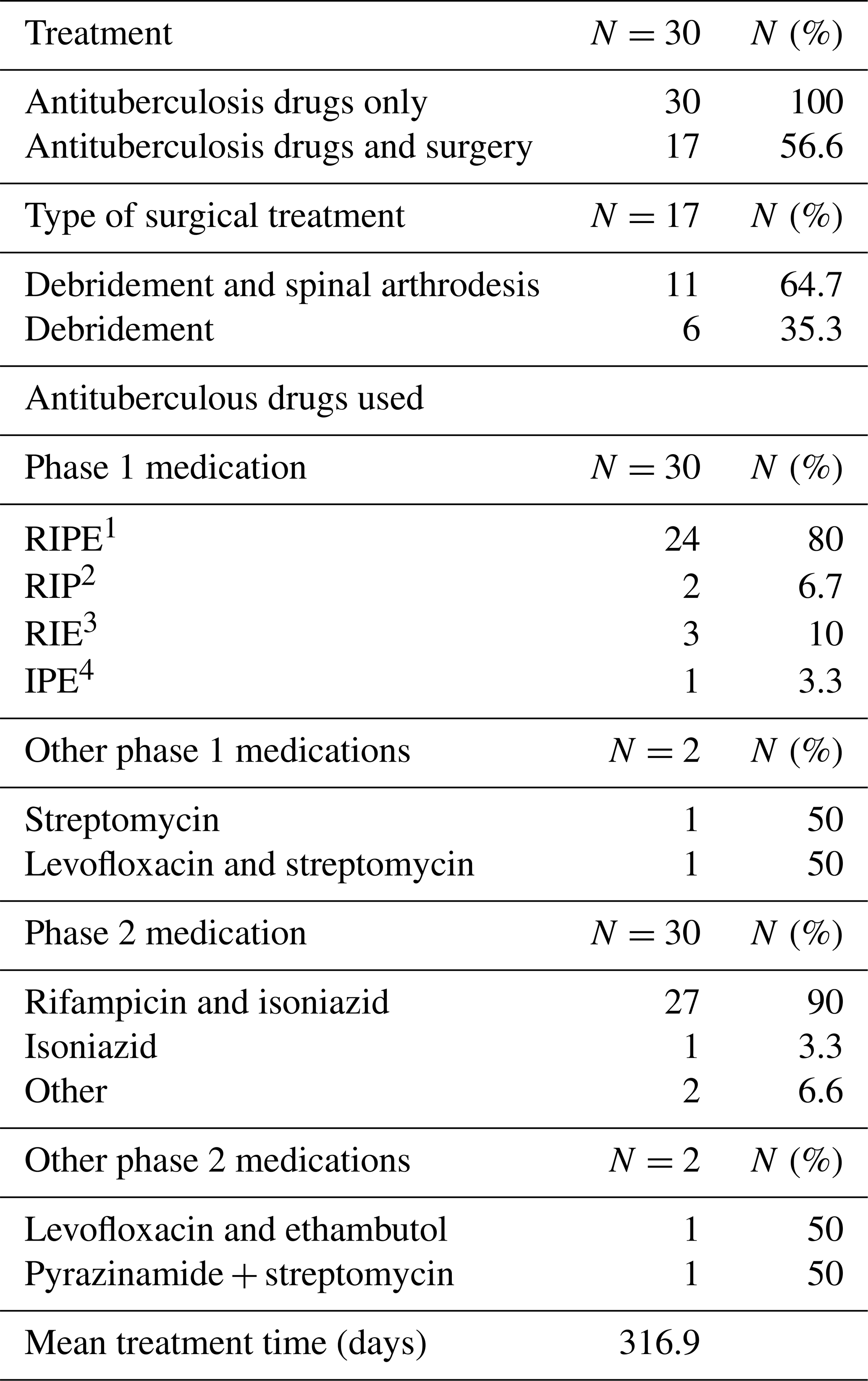
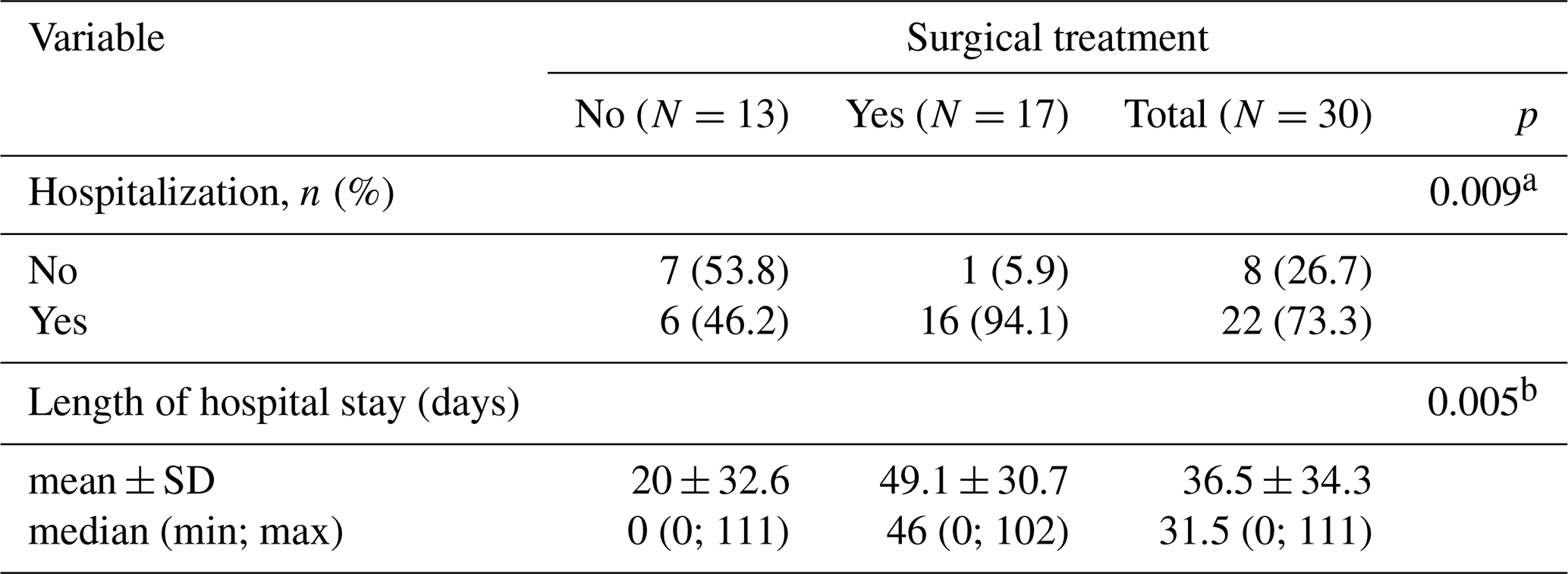
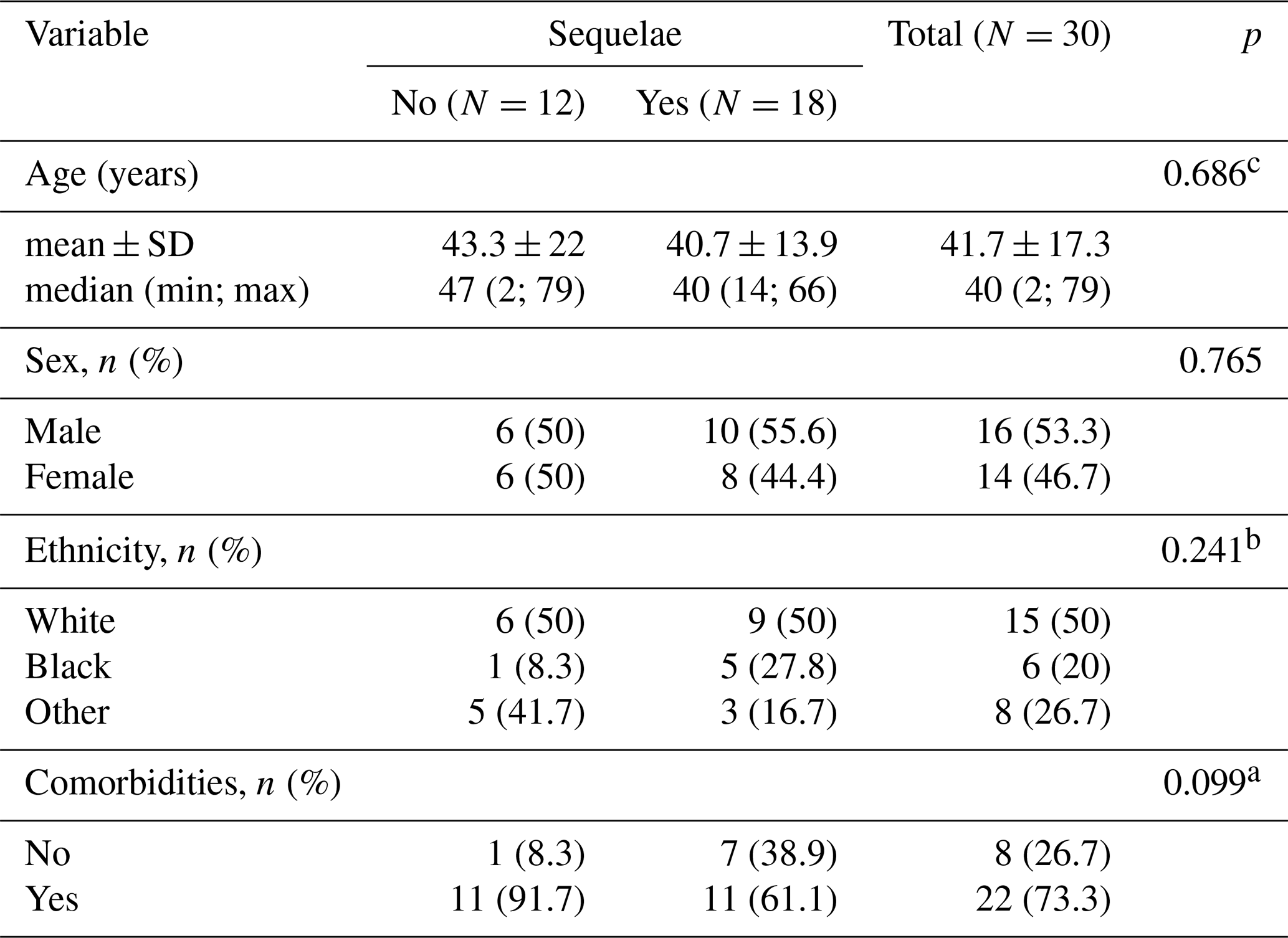
Introduction: tuberculosis (TB) remains a major cause of morbidity and mortality worldwide. The incidence of TB has increased since the 1980s. Given the increasing prevalence of TB worldwide, osteoarticular TB (OATB) is a significant health problem. Methods: retrospective study of a case series of hospitalized patients with confirmed OATB by culture or histopathological examination who were seen at a reference orthopedic hospital in São Paulo, Brazil, from 2014 to 2019. Results: thirty patients with confirmed bone and joint TB were seen from 2014 to 2019. The main sites of OATB were the spine (83.3 %) and the appendicular skeleton (26.7 %). Indication of surgical treatment was significantly related to the need for hospitalization (p=0.009) and the increased length of hospital stay (p=0.005). Presence of sequelae at the end of treatment was correlated with the presence of motor deficit at the time of OATB diagnosis (p=0.035) as well as with initial presence of functional limitation (p=0.025) and with high value of C-reactive protein at the end of treatment (p=0.037). Conclusions: the delay in the onset of clinical and laboratory signs of cases of osteoarticular infections hinders the early diagnosis and treatment of the disease, resulting in major complications sometimes requiring surgical treatment and consequently leading to a prolonged hospital stay, evidence of high inflammatory activities, and the presence of neurological deficits.