the Creative Commons Attribution 4.0 License.
the Creative Commons Attribution 4.0 License.
 | 18 May 2026
| 18 May 2026
The use of debridement, antibiotic pearls, and implant retention (DAPRI) in the management of acute periprosthetic joint infections: a systematic review
Doriana Di Costa
Giacomo Capece
Donato Coppola
Elena Matteini
Pierluigi Del Vecchio
Francesco Taccari
Giuseppe Maccagnano
Carlo Torti
Giulio Maccauro
Raffaele Vitiello
Background: Periprosthetic joint infection (PJI) represents one of the most severe complications following joint arthroplasty, largely due to bacterial biofilm formation on implant surfaces. While debridement, antibiotics and implant retention (DAIR) is commonly used for acute infections, its effectiveness remains variable. Debridement, antibiotic pearls and implant retention (DAPRI) has been proposed as a modified technique aimed at improving local antibiotic delivery and biofilm eradication. This systematic review evaluates the current evidence on the effectiveness and safety of DAPRI in PJI management. Materials and methods: A systematic review was conducted according to PRISMA guidelines. PubMed, Scopus and Web of Science databases were searched for studies reporting the use of DAPRI in adult patients with PJI. Eligible studies included retrospective studies and case series reporting surgical details and postoperative outcomes. Methodological quality was assessed using the MINORS score. Demographic data, microbiology, antibiotic regimens and clinical outcomes were analysed. Results: Five studies involving 128 patients met the inclusion criteria. The mean patient age was 69.4 years, with a mean follow-up of 22.4 months. PJIs involved the knee (n=78), hip (n=44) and shoulder (n=6). Gram-positive organisms predominated, with Staphylococcus aureus (32 %) and S. epidermidis (28.9 %) being the most frequently isolated pathogens. Infection eradication was achieved in 105 cases, corresponding to an overall success rate of 82 %. Twenty-three patients (18 %) required further surgical intervention. Reported complications were limited and included wound dehiscence, renal dysfunction and heterotopic ossification. Conclusions: DAPRI appears to be a promising implant-retention strategy for the treatment of PJI, showing encouraging infection eradication rates with a low incidence of complications. However, the current evidence is limited by small sample sizes, heterogeneity in patient selection, surgical technique and antibiotic protocols, as well as the lack of comparative studies. High-quality prospective trials are needed to better define the role of DAPRI relative to established surgical approaches.
- Article
(893 KB) - Full-text XML
- BibTeX
- EndNote




Hip and knee arthroplasties are among the most successful orthopaedic procedures, significantly improving patients' quality of life (Iorio et al., 2023). However, the rising number of primary arthroplasties has led to an increase in revision procedures, often due to complications such as periprosthetic joint infections (PJIs), which are among the most feared due to their high morbidity and mortality (Indelli et al., 2023; Ramos et al., 2026). PJIs can arise postoperatively, from microorganisms introduced during surgery; or haematogenously, originating from bloodstream infections. Periprosthetic joint infections are commonly classified by timing as early (within approximately 4 weeks after the index arthroplasty), delayed (between 4 and 24 months) and late (beyond 2 years, often haematogenous). In general, early or acute infections are associated with a relatively immature biofilm, whereas delayed and late infections are more often linked to a mature biofilm and a more indolent course (Ferrini et al. 2026; Vicenti et al., 2024).
One of the major challenges in PJI management is biofilm formation, which allows bacteria to persist on the implant surface, rendering them highly resistant to both systemic antibiotics and host immune responses. Due to the pivotal role of biofilm in sustaining infections, surgical intervention is often required. PJI treatment strategies include single-stage revision, 1.5-stage revision and two-stage revision; and debridement, antibiotics and implant retention (DAIR) (Iorio et al., 2023; Cashman et al., 2025). While prosthesis explantation is considered the gold standard, particularly in chronic cases, it is not always an optimal option for all patients.
DAIR is an alternative strategy for early postoperative or late haematogenous infections, with reported infection control rates ranging from 12 % to 80 % (Abbaszadeh et al., 2026). The highest success rates are seen in early infections (within 30 days of onset), low-virulence pathogens and healthy patients (Romanò et al., 2012; Warda et al., 2026). The DAIR procedure involves joint debridement, lavage, removal of interchangeable components and systemic antibiotic therapy tailored to culture results. Despite its advantages – being less invasive and preserving bone stock – DAIR has limitations, particularly in eradicating biofilm-related infections (Nurmohamed et al., 2021).
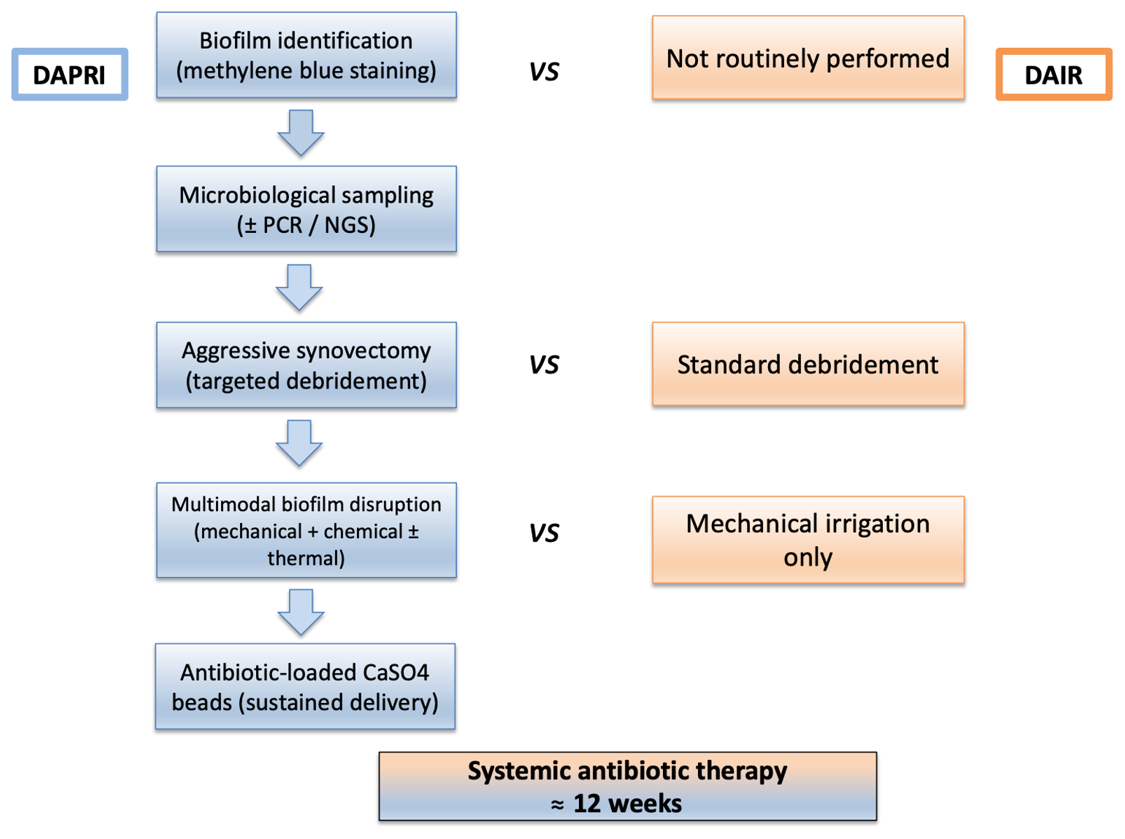
A modified approach, debridement, antibiotic pearls and implant retention (DAPRI) has been introduced to enhance local antibiotic delivery and improve infection eradication without prosthesis removal (Iorio et al., 2023; Indelli et al., 2023; Ghirardelli et al., 2020). DAPRI follows similar surgical steps to DAIR but incorporates microorganism isolation or identification, methylene blue staining for biofilm visualisation and aggressive synovectomy; mechanical, thermal and chemical biofilm disruption; and the use of resorbable antibiotic-loaded calcium sulfate beads for prolonged local antibiotic release (Shaw et al., 2017; Connaughton et al., 2014; Tria et al., 2018; Risitano et al., 2018). These beads, mixed with vancomycin, tobramycin and a third culture-specific antibiotic, provide sustained intra-articular drug delivery over 4–6 weeks (Risitano et al., 2018).
The DAPRI surgical approach for PJI involves three steps: biofilm identification, removal and recurrence prevention. Methylene blue stains the biofilm, guiding aggressive synovectomy. At this stage, biofilm is disrupted thermally (argon beam), mechanically (brushing with chlorhexidine) and chemically (pulse irrigation with bacitracin-added saline). A povidone-iodine soak and re-draping ensure sterility before implant placement. Antibiotic-loaded calcium sulfate beads provide localised treatment. Postoperatively, patients begin weight-bearing on day one and follow a 12-week antibiotic regimen (Connaughton et al., 2014; Tria et al., 2018; Risitano et al., 2018).
Although DAPRI theoretically enhances infection control by increasing local antibiotic concentration and biofilm removal, evidence remains limited. Some studies suggest improved outcomes over DAIR, particularly in cases with highly resistant biofilm formation (Zhang et al., 2020). However, long-term efficacy remains uncertain, and DAPRI is not yet widely included in clinical guidelines due to limited data from small cohort studies (Casiraghi et al., 2023). On the other side, the experts from the 2025 International Consensus Meeting (ICM) on PJIs have recommended a “DAPRI-like” surgical protocol for patients who have an acute periprosthetic joint infection (Cashman et al., 2025). No direct comparative studies exist between DAPRI and other surgical techniques.
This systematic review aims to assess whether DAPRI is an effective treatment option for early postoperative and acute haematogenous PJI.
This systematic review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guideline to ensure a rigorous and transparent methodology for data collection and analysis (Fig. 1).
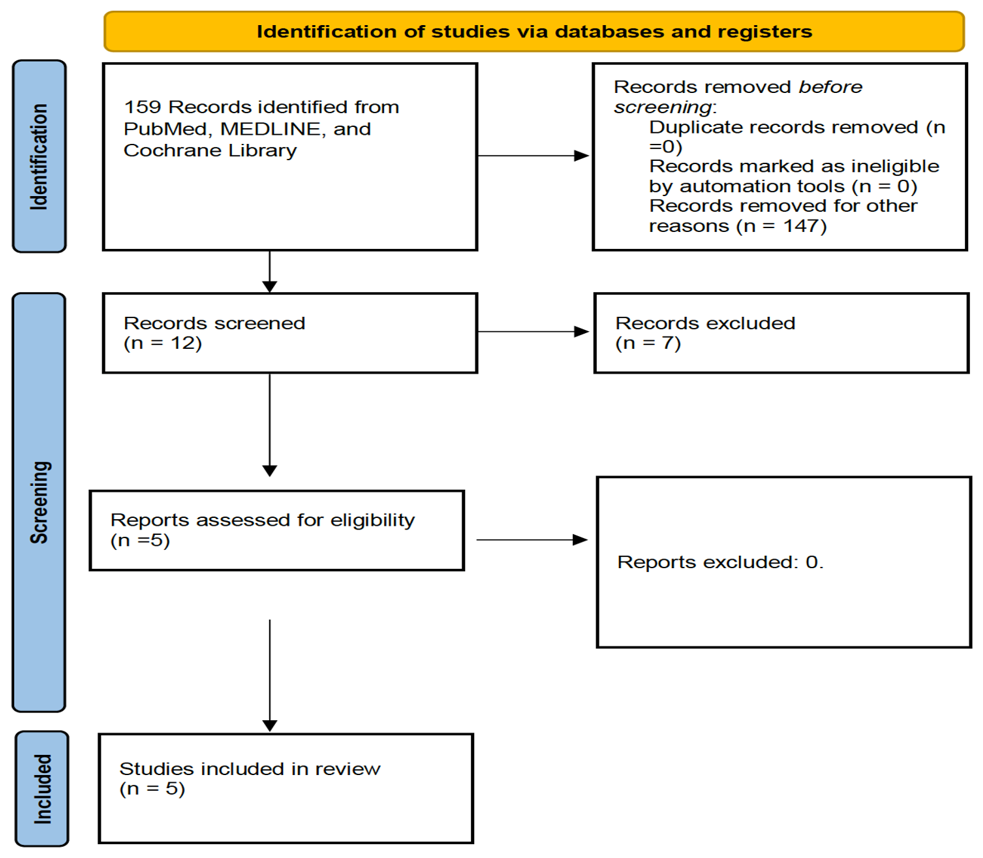
Figure 1PRISMA 2020 flow diagram for new systematic reviews, which included searches of databases and registers only.
2.1 Search strategy
A comprehensive literature search was performed across three major electronic databases: PubMed, Scopus and Web of Science. The search strategy included the keywords “Debridement antibiotic pearls and retention of the implant” and/or “DAPRI”. No filters or restrictions were applied to language or publication date to minimise the risk of excluding relevant studies. Titles and abstracts of all retrieved articles were independently screened by two authors (Doriana Di Costa and Giacomo Capece) to assess eligibility. In cases of uncertainty, the full text was obtained for detailed review. Discrepancies between reviewers were resolved by discussion and, when necessary, by consultation with a senior author (Raffaele Vitiello or Giulio Maccauro). Additionally, the reference lists of included articles were manually searched to identify further relevant studies that may have been missed during the initial database search. Articles were eligible for inclusion if they involved adult human subjects, were published in English and reported on the use of the DAPRI technique for the treatment of periprosthetic joint infection (PJI), with explicit description of the surgical procedure and postoperative outcomes. Journal names, author identities and institutional affiliations were not blinded at any stage of the selection process. The final set of included studies was retrospectively analysed by three authors (Doriana Di Costa, Giacomo Capece and Donato Coppola), who extracted the relevant data into a structured Microsoft Excel worksheet. This dataset was subsequently reviewed and validated by four authors (Raffaele Vitiello, Elena Matteini, Pierluigi Del Vecchio and Francesco Taccari) to ensure consistency and accuracy.
2.2 Inclusion and exclusion criteria
Studies were included based on the following criteria: (1) involvement of patients affected by PJI treated using the DAPRI protocol, (2) clear description of the surgical procedure performed, (3) reporting of postoperative outcomes and (4) availability of the full-text article. Additionally, we also decided to exclude articles focusing on DAIR, even when combined with local CaSo addition, in order to ensure greater homogeneity, therefore considering only studies that followed the fundamental key points of the DAPRI procedure. Both retrospective studies and case series were considered eligible. Exclusion criteria comprised review articles, technique notes, case reports, cadaveric or animal studies, and basic science research. Additionally, studies lacking outcome data or adequate follow-up were excluded. Three reviewers (Doriana Di Costa, Giacomo Capece and Elena Matteini) independently assessed the full texts of selected studies to determine eligibility and to extract data. In cases of disagreement, a final decision was reached by consensus or, if needed, with the input of a senior reviewer (Raffaele Vitiello). Risk of bias was independently evaluated by two authors (Donato Coppola and Elena Matteini) using predefined criteria, with disagreements resolved through discussion.
2.3 Data extraction and analysis
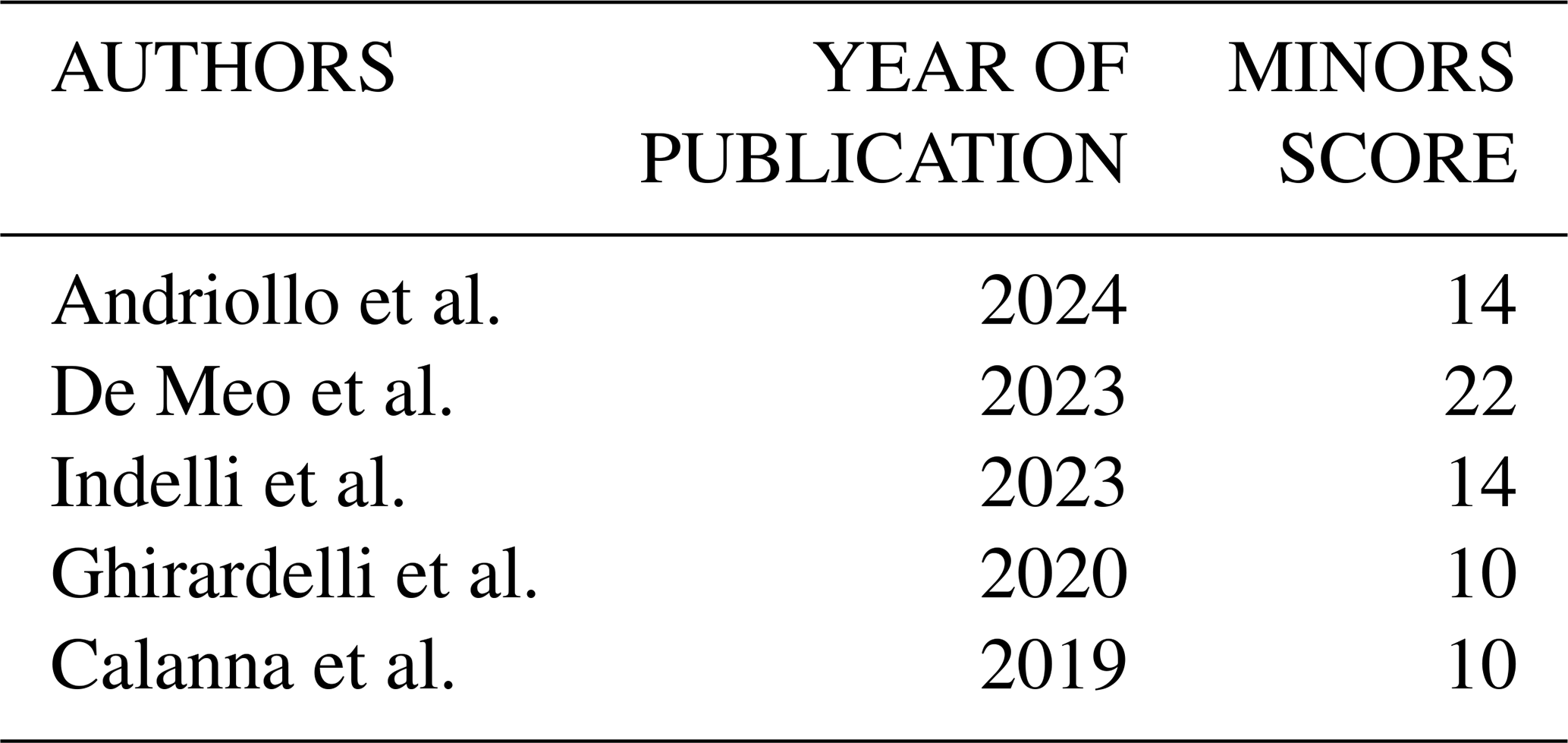
The methodological quality of the included studies was assessed using the Methodological Index for Non-Randomized Studies (MINORS) tool, which provides a maximum score of 16 for non-comparative studies and 24 for comparative studies. Two authors (Doriana Di Costa and Elena Matteini) independently assigned MINORS scores and reached consensus on the final ratings (Table 1). Data were analysed using SPSS software (SPSS, Inc., Chicago, IL, USA). Continuous variables are presented as means with standard deviations, while categorical variables are reported as frequencies and percentages. Statistical significance was set at p<0.05. For clarity and precision, all numerical values were rounded to one decimal place.
Table 1MINORS scores. 0–8 (non-comparative studies) or 0–12 (comparative studies): low methodological quality; 9–12 (non-comparative studies) or 13–18 (comparative studies): moderate methodological quality; 13–16 (non-comparative studies) or 19–24 (comparative studies): high methodological quality.
3.1 Demographic data, localisation, aetiology and microorganisms
A total of 159 articles were identified through the search. Following the PRISMA flowchart, five articles were considered relevant and were included in the final analysis (Fig. 1). According to the MINORS evaluation, the mean score of the studies reached was 14 points (10–22 points).
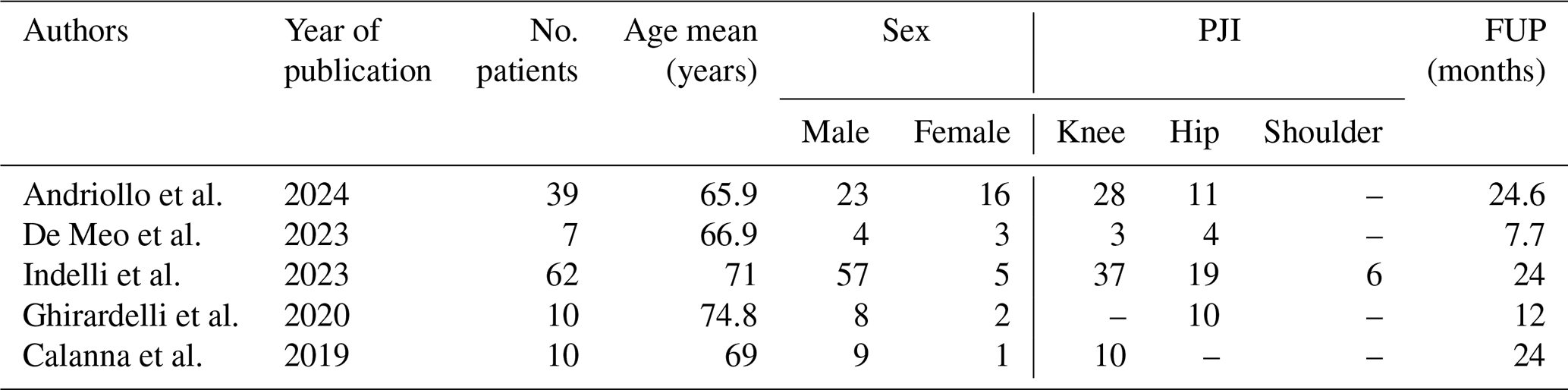
All patients included in the studies were diagnosed with acute PJI and underwent treatment with DAPRI. The studies collectively included a population of 128 patients: 101 were male and 27 were female. The average age of patients across the studies was 69.4 years and the mean follow-up was 22.4 months (range from 7.7 to 24.6). Of the included patients, 78 presented with a PJI of the knee, 44 of the hip and 6 of the shoulder. Among these cases, 34 were classified as postoperative PJIs and 12 as hematogenous PJIs, while the remaining cases were not further specified.
The predominant pathogens identified were Gram-positive bacteria (112 cases), followed by Gram-negative (15 cases), one fungal infection caused by Candida albicans and three cases with negative cultures. The most frequently isolated microorganism was Staphylococcus aureus (41), followed by S. epidermidis (37) and Escherichia coli (7). It was not always specified whether the infection was polymicrobial.
Table 3Isolated microorganisms; a NS: not specified; b others: Streptococcus sanguinis, Kocuria sp., Moraxella catarrhalis, Acinetobacter baumannii, Candida albicans, Enterobacter cloacae, Proteus mirabilis, Corynebacterium striatum, Granulicatella adiacens.

3.2 Selection of patients and choice of antibiotics for beads
3.2.1 Preparation
All patients underwent DAPRI surgery, with an average time between diagnosis of PJI and surgery of 8.8 d (range: 2 to 23.9 d). Andriollo et al. (2024) and Indelli et al. (2023) selected patients following the ICM 2018 criteria for DAIR. Indelli et al. (2023) specified that in culture-negative cases, additional diagnostic techniques such as multiplex PCR or next-generation sequencing were performed; they always performed an arthrocentesis before surgery in order to obtain a microbiological diagnosis. Ghirardelli et al. (2020) and Calanna et al. (2019) selected patients who had an acute postoperative infection (within 6 weeks of surgery) or a haematogenous infection, both with microorganism isolation. Notably, Ghirardelli et al. (2020) performed fluoroscopy-guided hip aspiration before surgery. De Meo et al. (2023) only mentioned that they considered patients with a diagnosis of DAPRI, without specifying the criteria used to make the diagnosis.
Except for De Meo et al. (2023), who did not provide precise data on the composition of the beads, in all other studies a 10 mL kit of PG-CSH (Stimulan; Biocomposites Ltd., UK) was used as the antibiotic carrier. Andriollo et al. (2024) added 1 g of powdered vancomycin and 0.24 g of liquid gentamicin solution or, if an antibiogram was available, a targeted antibiotic. Ghirardelli et al. (2020) and Calanna et al. (2019) added 1 g of powdered vancomycin, 0.8 g of liquid tobramycin solution and a third antibiotic depending on the isolated microorganism. Indelli et al. (2023) used unspecified antibiotics according to the antibiogram results. Additionally, Andriollo et al. (2024) and Indelli et al. (2023) incorporated an acetic acid benzalkonium chloride (BZK)-based surgical lavage solution (Bactisure, Zimmer Biomet, Warsaw, IN, USA) into their procedure.
Therefore, the most-used local antibiotic was vancomycin (27 patients), followed by gentamicin (14 patients) and tobramycin (10 patients). Less frequently, meropenem (one patient), amoxicillin combined with clavulanic acid (one patient) and amphotericin B (one patient) were used.
3.3 Systemic antibiotic therapy
Andriollo et al. (2024) did not specify the duration of postoperative antibiotic therapy but reported a range of 6–12 weeks. In the study by De Meo et al. (2023), patients received intravenous therapy for the duration of their hospital stay, with an average time of 27.4 d (range: 8 to 91 d), followed by 6 weeks of oral therapy. All other studies indicated that patients underwent 6 weeks of intravenous antibiotic therapy followed by 6 weeks of oral antibiotics.
De Meo et al. (2023) was the only study to specify the antibiotics used postoperatively. The most administered intravenous antibiotics were daptomycin (five patients), meropenem (two patients) and piperacillin/tazobactam (two patients), and a combination of anti-Gram-positive and anti-Gram-negative antibiotics were more frequently used. The study by Indelli et al. (2023) noted that the most commonly used intravenous antibiotics were glycopeptides and cephalosporins but did not provide precise data. Regarding oral antibiotics, in the study by De Meo et al. (2023), rifampicin and levofloxacin were the most frequently used combination (two patients). Indelli et al. (2023) also reported a preference for quinolones for oral therapy.
3.4 Outcomes
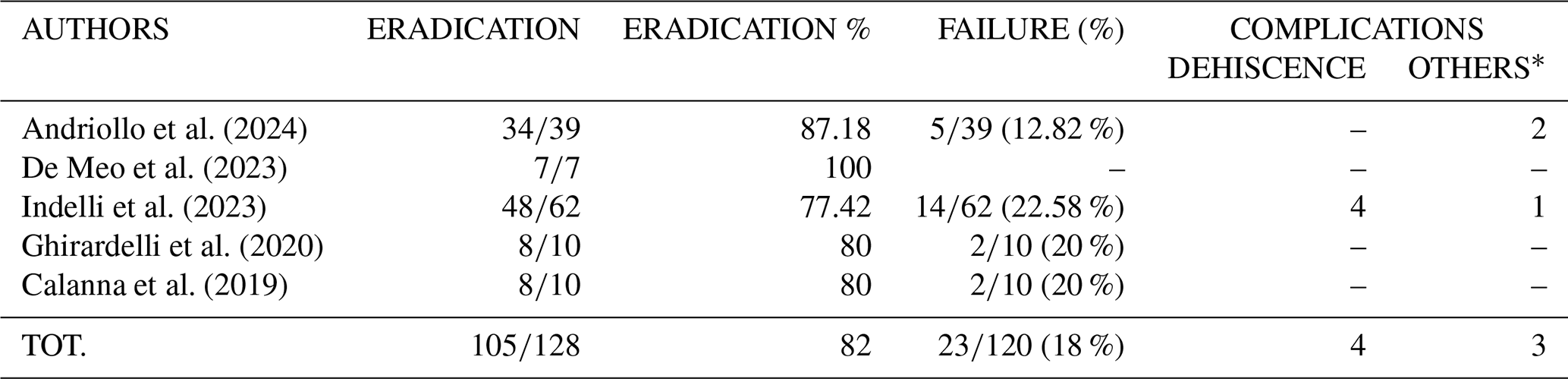
The studies reported 105 cases of infection eradication, corresponding to an eradication rate of 82 %. Conversely, 23 patients required a second surgery (two-stage revision). Only Andriollo et al. (2024) and Indelli et al. (2023) reported postoperative complications. Complications recorded included wound dehiscence (four patients), renal dysfunction (two patients), and heterotopic ossifications (one patient).
PJIs are among the most severe complications in orthopaedics, presenting complex management challenges and significant functional and psychological impacts on patients (Aggarwal et al., 2013). Despite their relatively low incidence, the rising prevalence of joint arthroplasty has made PJIs an increasing public health concern (Ayoade et al., 2025).
The results of this review indicate that DAPRI has been applied in a limited number of studies, with a total of 128 patients included. The reported eradication rate of 82 % appears promising; however, these findings must be interpreted cautiously due to a limited number of patients, heterogeneity in patient selection, diagnostic criteria and procedural details across studies. While most studies followed MSIS/ICM 2018 criteria for DAIR, others did not clearly specify inclusion thresholds (e.g. De Meo et al., 2023), limiting comparability and generalisability. Patient- and infection-related factors may also influence outcomes. Polymicrobial and fungal infections were inconsistently reported, and culture-negative cases lacked standardised management protocols. These gaps are particularly relevant, as polymicrobial infections and difficult-to-treat pathogens have been associated with higher failure rates (Wimmer et al., 2016). Future studies should systematically stratify outcomes according to infection type and consider tailored management strategies for culture-negative or fungal infections.
DAPRI should be considered a step-based implant-retention approach rather than a single procedure (Fig. 2). Across the available studies, several recurrent elements appear relevant for interpreting outcomes. The first is the isolation and identification of the microorganism, as this enables targeted antimicrobial therapy. Indelli et al. (2023) reported better results when DAPRI was performed in cases with microbiological identification compared with similar procedures performed without microorganism identification. In our review, except for De Meo et al. (2023) (where this step was not clearly reported), all other studies included microbiological assessment, although with different sampling methods. In line with this concept, Balato et al. (2022) also emphasise, in the broader DAIR literature, the importance of pathogen-oriented treatment and appropriate selection criteria as key determinants of success.
A second point relates to advanced diagnostics. Recent consensus recommendations support the use of molecular tests (e.g. PCR-based assays and next-generation sequencing) as an adjunct to conventional cultures to improve diagnostic accuracy and pathogen identification, particularly in culture-negative PJI and when rapid organism detection is clinically relevant (Martinazzi et al., 2025).
From a technical standpoint, most DAPRI protocols combine mechanical debridement, chemical adjuncts and, in some cases thermal- or energy-based steps, followed by local antibiotic delivery. In our review, the studies reported different intravenous-to-oral transition protocols and antibiotic choices (e.g. daptomycin vs glycopeptides), raising the possibility that some observed eradication rates reflect systemic therapy rather than DAPRI-specific efficacy. Likewise, technical heterogeneity in the DAPRI procedure itself – including differences in methylene blue staining, chemical debridement agents and bead composition – may have influenced outcomes. Calcium sulfate beads sometimes contained non-standardised additives (“third antibiotic” per surgeon preference), potentially confounding the apparent success rates. Vicenti et al. (2024) describe DAPRI as a multimodal debridement protocol combined with resorbable calcium sulfate antibiotic beads, and highlight that strict selection and protocol adherence are essential when implant retention is attempted.
Another key determinant is timing. Although major consensus documents refer to DAIR rather than DAPRI, DAPRI is based on the same implant-retention principles; therefore, it should be discussed within the acute PJI setting, where early intervention is recommended (Cashman et al., 2025; Gupta et al., 2024; Sigmund et al., 2025). Our findings are consistent with this concept, as the mean interval between diagnosis and treatment was 8.8 d. This is in line with Balato et al. (2022), who report that DAIR outcomes are more favourable when performed early after symptom onset, and with Vicenti et al. (2024), who describe DAPRI within strict “early/acute” indications. Vicenti et al. (2024) also highlighted the importance of prolonged systemic treatment, commonly reported as a 12-week course (approximately 6 weeks intravenous plus 6 weeks oral therapy, tailored to the antibiogram), which is consistent with recent recommendations to prolong systemic therapy following implant-retention procedures (Ferrini et al., 2026) to achieve better results.
Taken together, these comparisons may help to explain why our eradication rate was approximately 82 %. However, it remains unclear whether this difference is mainly driven by early timing and strict selection criteria, more consistent pathogen identification and targeted systemic therapy, the combined effect of mechanical/chemical/thermal debridement, local antibiotic delivery, or the combination of these factors.
Finally, applying all DAPRI steps may increase operative time and resource use, and this could make the procedure economically less favourable compared with standard DAIR; this aspect should be addressed in future comparative and cost-effectiveness studies.
Reported postoperative complications were limited, with only two studies documenting wound dehiscence (four cases) and renal dysfunction (two cases). The low complication rate is encouraging, but underreporting cannot be excluded and safety conclusions should remain cautious.
Follow-up duration represents another important limitation. The mean follow-up was 22.4 months, yet recurrences of PJI often occur beyond 2 years post-DAIR. Additionally, shoulder PJIs (n=6) were not separately analysed, despite known challenges related to biofilm formation in this joint. These factors highlight the need for long-term joint-specific outcome data.
Importantly, no included studies directly compared DAPRI to other surgical techniques such as DAIR or two-stage revision. Therefore, claims of superiority are not supported, and current evidence should be considered as preliminary or proof-of-concept. High-quality prospective randomised trials are urgently needed to evaluate DAPRI's comparative effectiveness, safety and long-term outcomes in both acute and chronic PJI management (Longo et al., 2024).
Several limitations of this review should be acknowledged. The first major limitation is represented by the quality of the analysed studies, with a mean MINORS score of 14, which highlights the need for high-quality comparative studies. The short and inconsistent follow-up across studies restricts assessment of long-term outcomes and late complications. The incomplete reporting of polymicrobial or fungal infections, culture-negative cases and postoperative complications limits the ability to fully evaluate the efficacy of DAPRI. Technical heterogeneity, including differences in bead composition, debridement methods and use of adjunctive agents, further limits comparability.
Collectively, these factors underscore the necessity for large, prospective and standardised studies to better define the role of DAPRI in PJI management.
Overall, the findings suggest that DAPRI may offer a promising alternative for PJI treatment, particularly in scenarios where implant retention is desired. Nevertheless, heterogeneity in patient selection, microbiological profiles, antibiotic regimens and procedural details currently limits definitive conclusions, and careful interpretation is warranted.
Future efforts should focus on defining specific criteria for patient selection, standardising surgical and postoperative protocols.
| DAIR | Debridement, antibiotics and implant retention |
| DAPRI | Debridement, antibiotic pearls and implant retention |
| IDSA | Infectious Diseases Society of America |
| MINORS | Methodological Index for Non-Randomized Studies |
| PJI | Periprosthetic joint infection |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
No datasets were generated or analysed in this systematic review. The search strategy is described in the materials and methods section.
All the authors approved the submitted version (and version substantially edited by journal staff that involves the authors' contribution to the study), and agree to be personally accountable for the authors' own contributions and for ensuring that questions related to the accuracy or integrity of any part of the work, even ones in which the authors were not personally involved, are appropriately investigated, resolved and documented in the literature. Conceptualisation and methodology: R.V. Validation: G.M. and C.T. Formal analysis: R.V. Investigation: D.D.C and G.C.. Writing (original draft preparation): D.D.C. and G.C. Writing (review and editing): D.D.C., G.C., D.C. and E.M.. Visualisation: G.M., C.T., F.T., P.D.V. and R.V. Supervision: G.M., C.T., F.T. and R.V. All authors have read and agreed to the published version of the paper.
The contact author has declared that none of the authors has any competing interests.
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of Orthopedic and Traumatology Institute of Università Cattolica del Sacro Cuore – Roma. As this is an approval from the Review Board of Orthopedic and Traumatology Institute, there is no code.
Publisher's note: Copernicus Publications remains neutral with regard to jurisdictional claims made in the text, published maps, institutional affiliations, or any other geographical representation in this paper. The authors bear the ultimate responsibility for providing appropriate place names. Views expressed in the text are those of the authors and do not necessarily reflect the views of the publisher.
Funded by the European Union – Next Generation EU – National Recovery and Resilience Plan (PNRR), Mission 6, Component 2 (M6C2), Investment 2.1: Enhancement and strengthening of biomedical research within the National Health Service (SSN) (grant no. PNRR-POC-2023-12378291).
This paper was edited by Derek Amanatullah and reviewed by two anonymous referees.
Abbaszadeh, A., Yilmaz, M. K., Izadi, N., Hoveidaei, A. H., Taheriazam, A., Abedi, A. A., and Parvizi, J.: Efficacy of Debridement, Antibiotics, and Implant Retention in Total Hip and Knee Arthroplasty: A Systematic Review and Meta-Analysis, J. Arthroplasty, 41, 19–38, https://doi.org/10.1016/j.arth.2025.05.121, 2026.
Aggarwal, V. K., Rasouli, M. R., and Parvizi, J.: Periprosthetic Joint Infection: Current Concept, Indian J. Orthop., 47, 10–17, https://doi.org/10.4103/0019-5413.106884, 2013.
Andriollo, L., Sangaletti, R., Velluto, C., Perticarini, L., Benazzo, F., and Rossi, S. M. P.: Impact of a Novel Antiseptic Lavage Solution on Acute Periprosthetic Joint Infection in Hip and Knee Arthroplasty, J. Clin. Med., 13, 3092, https://doi.org/10.3390/jcm13113092, 2024.
Ayoade, F., Li, D., Mabrouk, A., and Todd, J. R.: Periprosthetic Joint Infection, in: StatPearls, StatPearls Publishing, Treasure Island (FL), PMID: 28846340, 2025.
Balato, G., Ascione, T., De Matteo, V., Lenzi, M., Amato, M., De Giovanni, R., Festa, E., and Mariconda, M.: Debridement and Implant Retention in Acute Hematogenous Periprosthetic Joint Infection after Knee Arthroplasty: A Systematic Review, Orthop. Rev., 14, https://doi.org/10.52965/001c.33670, 2022.
Calanna, F., Chen, F., Risitano, S., Vorhies, J. S., Franceschini, M., Giori, N. J., and Indelli, P. F.: Debridement, Antibiotic Pearls, and Retention of the Implant (DAPRI): A Modified Technique for Implant Retention in Total Knee Arthroplasty PJI Treatment, J. Orthop. Surg., 27, 2309499019874413, https://doi.org/10.1177/2309499019874413, 2019.
Cashman, J., Falotico, G., Artyukh, V., Bagaria, V., Balato, G., Baron, G., Deckey, D., Hilton, T., Hipfl, C., Jones, C., Matthews, S., Nace, J., Springer, B., Winkler, T., and Yates, P.: 2025 ICM: Abbreviated Two- and 1.5-Stage, J. Arthroplasty, 41, S381–S384, https://doi.org/10.1016/j.arth.2025.10.075, 2025.
Cashman, J., Mortazavi, S. M. J., Indelli, P. F., Rele, S., Haasper, C., Yildiz, F., Holland, C. T., Lizcano, J. D., Auñón-Rubio, Á., Tai, D. B. G., Allende, B., Alvand, A., Arias, C., Arshi, A., Artyukh, V., Babis, G. C., Baeza-Oliete, J., Budhiparama, N., Buttacavoli, F., Carvalho, P. I., Vilchez Cavazos, F. C., Chen, C.-F., Chodór, P., Choong, P. F. M., Çiloglu, O., Dewar, D., Díaz, F. J., Dikmen, G., Ebied, A., Esmaeili, S., Evans, J. T., Falotico, G., Foguet, P., Franceschini, M., Gold, P., Gómez-Barrena, E., Gómez-Junyent, J., Gould, D., Hammad, A. A., Han, H.-S., Hipfl, C., Hunter, C., Incesoy, M. A., Kaplan, N. B., Karaytug, K., Li, H., Linares, F. A., Manrique-Succar, J., Marín-Peña, O., McCarroll, P., McCulloch, R., Mihalič, R., Morata, L., Mortazavi, S. A., Nandi, S., Naufal, E., Palacios, J. C., Martinez Pastor, J. C., Petheram, T., Ritter, A., Rolfson, O., Ros, J. M., Sanchez, M., Sancho, I., Shah, J. D., Sheng, P., Soriano, A., Spangehl, M. J., Stambough, J. B., Tarabichi, S., Taupin, D., Thiengwittayaporn, S., Tözün, I. R., Trebše, R., Tsai, S.-W., Tuncay, I., Veltman, E. S., Vilchez-Cavazos, F., Westberg, M., Wu, H., Yates, P. J., Yilmaz, M. K., and Yoo, J.-H.: 2025 ICM: Debridement, Antibiotics, and Implant Retention, J. Arthroplasty, 41, S297–S325, https://doi.org/10.1016/j.arth.2025.10.076, 2025.
Casiraghi, A., Galante, C., Rohayem, M., Vittone, G., Domenicucci, M., Cattaneo, S., Paderno, M., Grava, G., Van Hauwermeiren, E., and Milano, G.: Implant Retention with Serial Debridement and Use of Antibiotic-Loaded Calcium Sulfate Beads in Acute Fracture-Related Infection (FRI) after Pelvic Ring or Acetabular Fractures: A Retrospective Case Series of 7 Cases, Injury, 54, 1082–1087, https://doi.org/10.1016/j.injury.2023.01.045, 2023.
Connaughton, A., Childs, A., Dylewski, S., and Sabesan, V. J.: Biofilm Disrupting Technology for Orthopedic Implants: What's on the Horizon?, Front. Med., 1, https://doi.org/10.3389/fmed.2014.00022, 2014.
De Meo, D., Martini, P., Pennarola, M. F., Guarascio, G., Rivano Capparuccia, M., Iaiani, G., Candela, V., Gumina, S., and Villani, C.: Hydrogel Coating versus Calcium Sulphate Beads as a Local Antibiotic Carrier for Debridement Procedures in Acute Periprosthetic Joint Infection: A Preliminary Study, Gels, 9, 758, https://doi.org/10.3390/gels9090758, 2023.
Ferrini, A., He, M., Bernaus, M., Veloso, M., Mont, M. A., and Parvizi, J.: International Consensus Meeting on Orthopaedic Infection: Differences Between ICM 2018 and ICM 2025, J. Arthroplasty, 41, 304–307, https://doi.org/10.1016/j.arth.2025.10.113, 2026.
Ghirardelli, S., Fidanza, A., Prati, P., Iannotti, F., and Indelli, P. F.: Debridement, Antibiotic Pearls, and Retention of the Implant in the Treatment of Infected Total Hip Arthroplasty, HIP Int., 30 (1_suppl), 34–41, https://doi.org/10.1177/1120700020929314, 2020.
Gupta, V., Shahban, S., Petrie, M., Kimani, P. K., Kozdryk, J., Riemer, B., King, R., Westerman, R., and Foguet, P.: DAIR for Periprosthetic Joint Infections – One Week to Save the Joint?, Arthroplasty, 6, 61, https://doi.org/10.1186/s42836-024-00282-y, 2024.
Indelli, P., Ghirardelli, S., Valpiana, P., Bini, L., Festini, M., and Iannotti, F.: Debridement, Antibiotic Pearls, and Retention of the Implant (DAPRI) in the Treatment of Early Periprosthetic Joint Infections: A Consecutive Series, Pathogens, 12, 605, https://doi.org/10.3390/pathogens12040605, 2023.
Iorio, R., Iannotti, F., Previ, L., Viglietta, E., Gugliotta, Y., Corsetti, F., Fenucci, S., De Carli, A., Indelli, P. F., and Redler, A.: A Modified Technique for Two-Stage Revision in Knee PJI Treatment, J. Clin. Med., 12, 7323, https://doi.org/10.3390/jcm12237323, 2023.
Longo, U. G., De Salvatore, S., Bandini, B., Lalli, A., Barillà, B., Budhiparama, N. C., and Lustig, S.: Debridement, Antibiotics, and Implant Retention (DAIR) for the Early Prosthetic Joint Infection of Total Knee and Hip Arthroplasties: A Systematic Review, J. ISAKOS, 9, 62–70, https://doi.org/10.1016/j.jisako.2023.09.003, 2024.
Martinazzi, B. J., Indelli, P. F., Azboy, I., Babis, G., Dikmen, G., Flores, H., Franceschini, M., Goswami, K., Han, H.-S., Huddleston, J., Kobayashi, N., Krsak, M., Kruczyński, J., Lee, M., Lima, A. L. M., Mitton, B. C., Natesan, R., Neyt, J. G., and Portillo, M. E.: 2025 ICM: Diagnostic Techniques: Molecular Tests, J. Arthroplasty, 41, S407–S411, https://doi.org/10.1016/j.arth.2025.10.085, 2025.
Nurmohamed, F. R. H. A., van Dijk, B., Veltman, E. S., Hoekstra, M., Rentenaar, R. J., Weinans, H. H., Vogely, H. C., and van der Wal, B. C. H.: One-year infection control rates of a DAIR (debridement, antibiotics and implant retention) procedure after primary and prosthetic-joint-infection-related revision arthroplasty – a retrospective cohort study, J. Bone Joint Infect., 6, 91–97, https://doi.org/10.5194/jbji-6-91-2021, 2021.
Ramos, M. S., Benyamini, B., Kompala, V., Khan, S. T., Kunze, K. N., Visperas, A., Surace, P. A., and Piuzzi, N. S.: Mortality after an Infected Total Knee Arthroplasty: A Meta-Analysis, Bone Jt. J., 108-B, 177–184, https://doi.org/10.1302/0301-620X.108B2.BJJ-2025-0106.R1, 2026.
Risitano, S., Sabatini, L., Atzori, F., Massè, A., and Indelli, P. F.: Static Antibiotic Spacers Augmented by Calcium Sulphate Impregnated Beads in Revision TKA: Surgical Technique and Review of Literature, J. Orthop., 15, 313–318, https://doi.org/10.1016/j.jor.2018.02.008, 2018.
Romanò, C. L., Manzi, G., Logoluso, N., and Romanò, D.: Value of Debridement and Irrigation for the Treatment of Peri-Prosthetic Infections. A Systematic Review, HIP Int., 22 (8_suppl), 19–24, https://doi.org/10.5301/HIP.2012.9566, 2012.
Shaw, J. D., Miller, S., Plourde, A., Shaw, D. L., Wustrack, R., and Hansen, E. N.: Methylene Blue–Guided Debridement as an Intraoperative Adjunct for the Surgical Treatment of Periprosthetic Joint Infection, J. Arthroplasty, 32, 3718–3723, https://doi.org/10.1016/j.arth.2017.07.019, 2017.
Sigmund, I. K., Wouthuyzen-Bakker, M., Ferry, T., Metsemakers, W.-J., Clauss, M., Soriano, A., Trebse, R., and Sousa, R.: Debridement, antimicrobial therapy, and implant retention (DAIR) as curative surgical strategy for acute periprosthetic hip and knee infections: a summary of the position paper from the European Bone & Joint Infection Society (EBJIS), J. Bone Joint Infect., 10, 139–142, https://doi.org/10.5194/jbji-10-139-2025, 2025.
Tria, A. J., Scuderi, G. R., Cushner, F. D.: Complex Cases in Total Knee Arthroplasty: A Compendium of Current Techniques, Springer International Publishing, Cham, Switzerland, https://doi.org/10.1007/978-3-319-69380-4, 2018.
Vicenti, G., Pesare, E., Colasuonno, G., Buono, C., Albano, F., Ladogana, T., Passarelli, A. C., and Solarino, G.: Debridement, Antibiotic Pearls, and Retention of the Implant (DAPRI) in the Treatment of Early Periprosthetic Knee Joint Infections: A Literature Review, Healthcare, 12, 843, https://doi.org/10.3390/healthcare12080843, 2024.
Warda, H., Suliman, J., Chakhide, M., and Samaan, M.: Review of Recent Advances in Managing Periprosthetic Joint Infection After Total Knee Arthroplasty: DAIR Technique, Orthop. Res. Rev., 18, 1–14, https://doi.org/10.2147/ORR.S567611, 2026.
Wimmer, M. D., Friedrich, M. J., Randau, T. M., Ploeger, M. M., Schmolders, J., Strauss, A. A., Hischebeth, G. T. R., Pennekamp, P. H., Vavken, P., and Gravius, S.: Polymicrobial Infections Reduce the Cure Rate in Prosthetic Joint Infections: Outcome Analysis with Two-Stage Exchange and Follow-up ≥ two Years, Int. Orthop., 40, 1367–1373, https://doi.org/10.1007/s00264-015-2871-y, 2016.
Zhang, C., He, L., Fang, X., Huang, Z., Bai, G., Li, W., and Zhang, W.: Debridement, Antibiotics, and Implant Retention for Acute Periprosthetic Joint Infection, Orthop. Surg., 12, 463–470, https://doi.org/10.1111/os.12641, 2020.