the Creative Commons Attribution 4.0 License.
the Creative Commons Attribution 4.0 License.
 | 09 Apr 2026
| 09 Apr 2026
Is there a role for lavage aspiration after a dry tap in the work-up for potential periprosthetic joint infection? A systematic review
Sander Bruyninckx
Stijn Ghijselings
Melissa Depypere
Alex Soriano
Willem-Jan Metsemakers
Georges Vles
Aim: Lavage aspiration following a dry tap remains a debated technique in the work-up for periprosthetic joint infection (PJI) of the hip and knee. This systematic review critically appraises the available evidence, with a particular focus on the diagnostic yield of lavage aspiration in detecting PJIs that would otherwise be missed. Methods: A comprehensive literature search was conducted in accordance with PRISMA guidelines across PubMed, Embase, MEDLINE, and Cochrane databases. Results: Eleven studies met the inclusion criteria, all level IV case series. Across 1965 patients, 2199 aspirations were performed. Overall, 798 procedures (36 %) resulted in a dry tap. Lavage aspiration was attempted in 698 of these cases, with 691 successful attempts. Among dry taps, 154 PJIs were ultimately identified, corresponding to a PJI prevalence of 19 %. Lavage aspiration contributed to a correct diagnosis in 22 % of successful procedures. Pooled culture sensitivity and specificity following saline lavage were 66 % and 89 %, respectively. The diagnostic performance of polymorphonuclear neutrophils (PMNs) >80 % was similar between saline lavage and normal aspiration. Although no safety concerns were reported, the potential introduction of pathogens and the risk of false-positive results remain concerns that are not fully mitigated by the available evidence. Conclusion: One in three aspirations result in a dry tap. Lavage aspiration provides analysable fluid in nearly all cases and appears to enable the diagnosis of PJI in roughly one out of five patients in whom standard aspiration fails. However, more robust evidence is needed before it can be recommended as a universal technique.
- Article
(1260 KB) - Full-text XML
- BibTeX
- EndNote




Successful treatment of a patient with a potential periprosthetic joint infection (PJI) starts with a correct diagnosis as both over- and under-treatment can have severe consequences. The workhorse in the diagnostic process is the image-guided arthrocentesis, after which synovial fluid is sent for diagnostic testing. According to the 2021 European Bone & Joint Infection Society (EBJIS) criteria, a PJI is present in case the synovial fluid contains over 3000 white blood cells (WBCs) per microlitre, of which over 80 % are polymorphonuclear neutrophils (PMNs) or when alpha-defensin testing is positive (McNally et al., 2021). Identification of highly pathogenic micro-organisms, such as Staphylococcus aureus or Gram-negative rods, is also considered strongly indicative of infection. The confirmation or exclusion of a PJI beforehand offers several advantages. Beyond being essential for selecting the correct surgical treatment strategy, it also allows for adequate patient counselling, estimating operating time, and the correct use of antibiotics.
Unfortunately, not all joint aspirations yield (sufficient) synovial fluid. It is estimated that these so-called dry taps are encountered in one out of three cases (Roberts et al., 1992; Mulcahy et al., 1996; Somme et al., 2003; Ali et al., 2006; Partridge et al., 2018; Barker et al., 2021; Christensen et al., 2022; Treu et al., 2023). Reasons for not being able to aspirate joint fluid include inadequate technique, premature ending of the procedure due to discomfort for the patient, the fluid being too thick to pass through to the needle, or debris clogging the needle as soon as aspiration is attempted (Fig. 1).
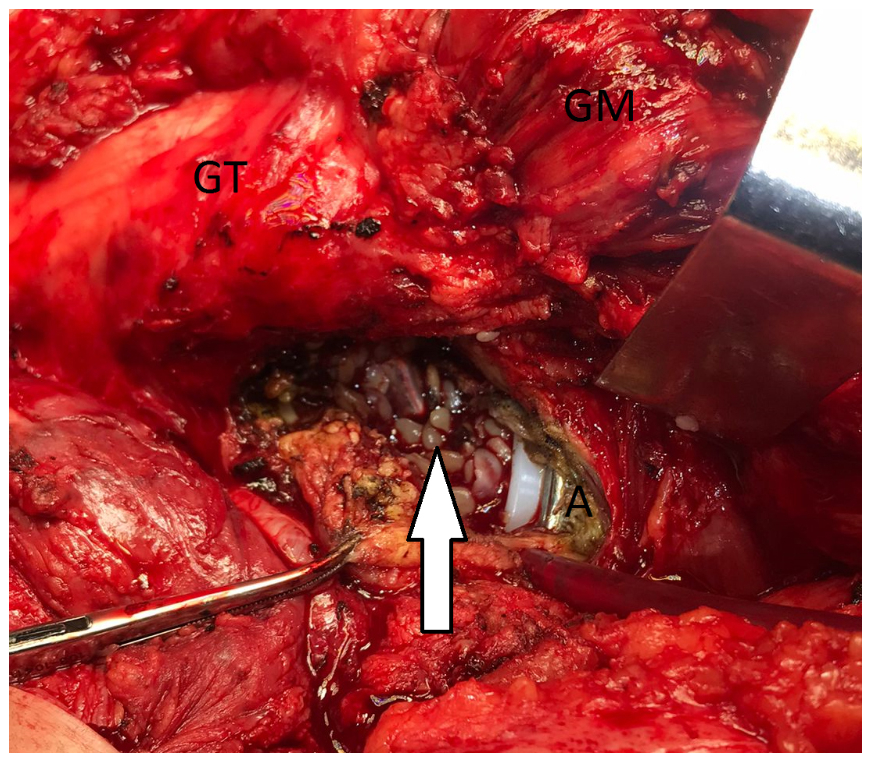
Figure 1Intra-operative photograph during a revision for a PJI of a THA. A pre-operative arthrocentesis yielded a dry tap, which was followed by a lavage aspiration that led to the identification of Staphylococcus epidermidis. An intra-operative aspiration again led to a dry tap. After the posterior arthrotomy, it was found that numerous flakes occupied the joint space (white arrow), which probably clogged the needle during attempted aspiration. Four out of six intra-operative samples were again positive for S. epidermidis PJI. GT – greater trochanter, GM – gluteus medius, A – acetabulum.
Importantly, a dry tap does not exclude the presence of infection. Studies have shown that PJI was present in 14 % of patients who had a pre-operative dry tap (Serfaty et al., 2022). Efforts should therefore be made to avoid these unsuccessful joint aspirations. Measures should include using image guidance such as fluoroscopy or ultrasound, providing adequate analgesia and sedation when the procedure turns out to be painful for the patient, and having the procedure performed by an experienced surgeon or radiologist. Another, but controversial, method to deal with a dry tap is the so-called saline lavage aspiration. In this procedure, saline is injected into the artificial joint and the proportion of fluid that can be re-aspirated is sent for diagnostic testing. Despite some promising studies, the 2025 International Consensus Meeting (ICM) on Musculoskeletal Infection (Istanbul) advised against performing lavage aspiration after a dry tap (Burgo et al., 2025). This recommendation was primarily based on the limited and heterogeneous evidence available, the absence of a standardised technique, and concerns about potential false-positive results and iatrogenic infections. The lack of standardisation represents a modifiable limitation that could be addressed through clear guidance from international expert bodies such as the ICM and EBJIS.
Joint aspiration and intra-articular injection are inherently invasive procedures that carry some procedural risks when performed in the setting of total hip arthroplasty (THA) and total knee arthroplasty (TKA), most notably the risk of iatrogenic PJI. However, when performed under strict aseptic conditions by an experienced clinician, this risk appears to be extremely low. In a retrospective analysis of 133 diagnostic knee aspirations in 115 TKAs, Keating et al. (2023) reported no cases of iatrogenic PJIs or aspiration-related complications over 6 months of follow-up. Similarly, Rajakulasingam et al. (2021) observed no iatrogenic PJIs or post-procedural complications across 111 synovial aspiration and biopsy procedures in a cohort of 103 THA and TKA patients followed for 1 year. The absence of observed events in these studies should not be interpreted as evidence that the true risk is zero. A nationwide epidemiological study from Iceland estimated the incidence of septic arthritis following arthrocentesis at approximately 0.037 % per procedure (Geirsson et al., 2008), and other cohort studies evaluating arthrocentesis and intra-articular injections have likewise reported very low but measurable rates, generally below 0.1 % (Petersen et al., 2019). The risk may be further amplified in the context of prosthetic joints, as the minimal infecting dose is more than 10 000-fold lower in the presence of an implant than in its absence (Zimmerli et al., 1982).
By contrast, intra-articular corticosteroid injection (IACI) into prosthetic joints has been associated with a significantly elevated risk of PJI. Across both TKA and unicompartmental knee arthroplasty (UKA) populations, reported PJI rates following IACI range from 1.3 % to 2.7 % in injected patients, compared to 0.8 % to 1.3 % in non-injected controls (Mills et al., 2018; Roecker et al., 2020; Durst et al., 2023; Rodriguez et al., 2023).
Arguably, the risks of saline lavage will probably be slightly higher than a plain joint aspiration but significantly lower than corticosteroid injections and should be weighed against the risks of missing the diagnosis of PJI before revision surgery.
Ultimately, the validity of the current recommendation depends on balancing the potential reduction in diagnostic accuracy due to dilution of the synovial fluid sample against the serious consequences of missing a PJI prior to revision surgery.
In this systematic review, we aim to critically evaluate the role of lavage aspiration after a dry tap in the work-up of PJI. We are particularly interested in the frequency that lavage aspiration leads to the diagnose of PJI, which would otherwise have been missed. Other outcomes investigated are the predictive values of lavage aspiration and its safety profile.
2.1 Search strategy
A comprehensive literature search was conducted on 1 April 2025 in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Databases searched included PubMed, Scopus, Embase, MEDLINE, and Cochrane. The following freetext keywords were used: (lavage OR reaspiration OR dry tap OR arthrocentesis) AND ((peri)prosthetic joint infection OR PJI). Conference abstracts and preprints were excluded from the search. Only full-text articles published in English were considered, with no restrictions on publication date. Reference lists of included studies were manually screened to identify additional eligible articles. Prior to the search, the study protocol was registered in the PROSPERO international prospective register of systematic reviews (ID no. 1024609).
2.2 Eligibility criteria
After the removal of duplicates, all records were screened independently by two reviewers (SB, GV), who were not blinded to study authorship or journal of publication. Studies were included if they (1) involved an adult population (≥18 years), (2) reported on at least five patients who underwent lavage aspiration after dry tap, and (3) met minimum quality standards (see below).
2.3 Quality assessment
Study quality was assessed using the National Institutes of Health (NIH) Quality Assessment Tool for Case Series. Only studies scoring ≥6 were included. Risk of bias assessment was performed independently by two reviewers (SB, GV), with disagreements resolved by consensus.
2.4 Definition of PJI
As no standardised definition of PJI was uniformly reported across studies, the diagnostic criteria provided by each study were accepted as presented. Intra-operative culture results were generally used as the primary determinant. Eight studies defined PJI as two positive cultures with the same organism (Mulcahy et al., 1996; Somme et al., 2003; Ali et al., 2006; Newman et al., 2017; Li et al., 2019; Heckmann et al., 2020; Christensen et al., 2022; Treu et al., 2023), while three studies required three positive cultures with the same organism (Roberts et al., 1992; Partridge et al., 2018; Barker et al., 2021). A single positive culture was considered probable contamination. No distinction was made between acute and chronic PJIs.
2.5 Data extraction and outcomes
From each included study, data were extracted on sample size, demographic characteristics, type of intervention, and relevant outcome parameters. The primary outcome was the frequency of PJI diagnosis following lavage aspiration after initial dry tap. Secondary outcomes included diagnostic performance of synovial fluid parameters (WBC count >3000 µL−1, PMN percentage >80 %, and culture results) as well as reported complications and safety concerns. The culture results of the lavage aspiration were regarded as true positive if it demonstrated concordance with the culture findings from intra-operative specimens in nine studies (Roberts et al., 1992; Mulcahy et al., 1996; Somme et al., 2003; Ali et al., 2006; Newman et al., 2017; Partridge et al., 2018; Barker et al., 2021; Christensen et al., 2022; Treu et al., 2023). Heckmann et al. (2020) compared the culture results of pre- and post-lavage aspirations.
As indicated in Table 3, (some of) the diagnostic characteristics in seven studies were calculated based on the raw data reported in each study (Roberts et al., 1992; Mulcahy et al., 1996; Somme et al., 2003; Heckmann et al., 2020; Barker et al., 2021; Christensen et al., 2022; Treu et al., 2023).
2.6 Statistical analysis
Descriptive analyses were performed using IBM SPSS Statistics version 28 (Armonk, NY, USA).
3.1 Studies included
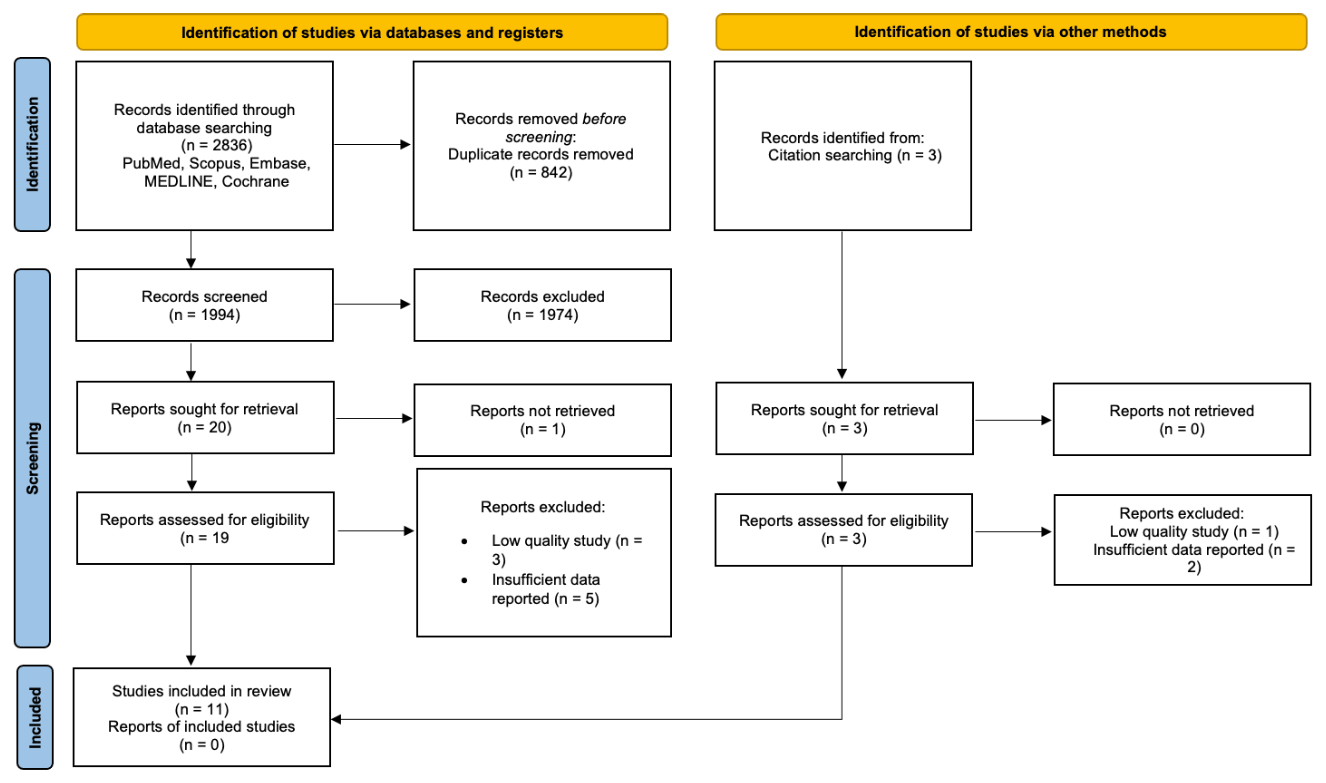
A total of 2836 records were identified (2833 through database searches and three through manual reference list screening). After the removal of duplicates and title/abstract screening, 19 full-text articles were assessed for eligibility. Eight failed to meet the inclusion criteria, leaving 11 studies for final analysis (Fig. 2). Of these, five applied the (modified) Musculoskeletal Infection Society (MSIS) International Consensus Meeting (ICM) criteria and one applied the European Bone and Joint Infection Society (EBJIS) criteria for the diagnosis of PJI.
3.2 Quality assessment
No randomised controlled trials were identified. All included studies were case series (level IV evidence) and achieved a score ≥6 on the NIH Quality Assessment Tool for Case Series, with a mean score of 7.5 (Table 1). Study quality was limited by retrospective design; small sample sizes (7 of 11 studies reported <50 lavage aspirations); the absence of controls or comparator groups; potential selection bias; and methodological heterogeneity regarding needle size, aspiration technique, and outcome measures.
Table 1Study characteristics and quality rating.

N – sample size; NIH – National Institutes of Health Quality Assessment Tool; CT – computed tomography.
3.3 Patient demographics
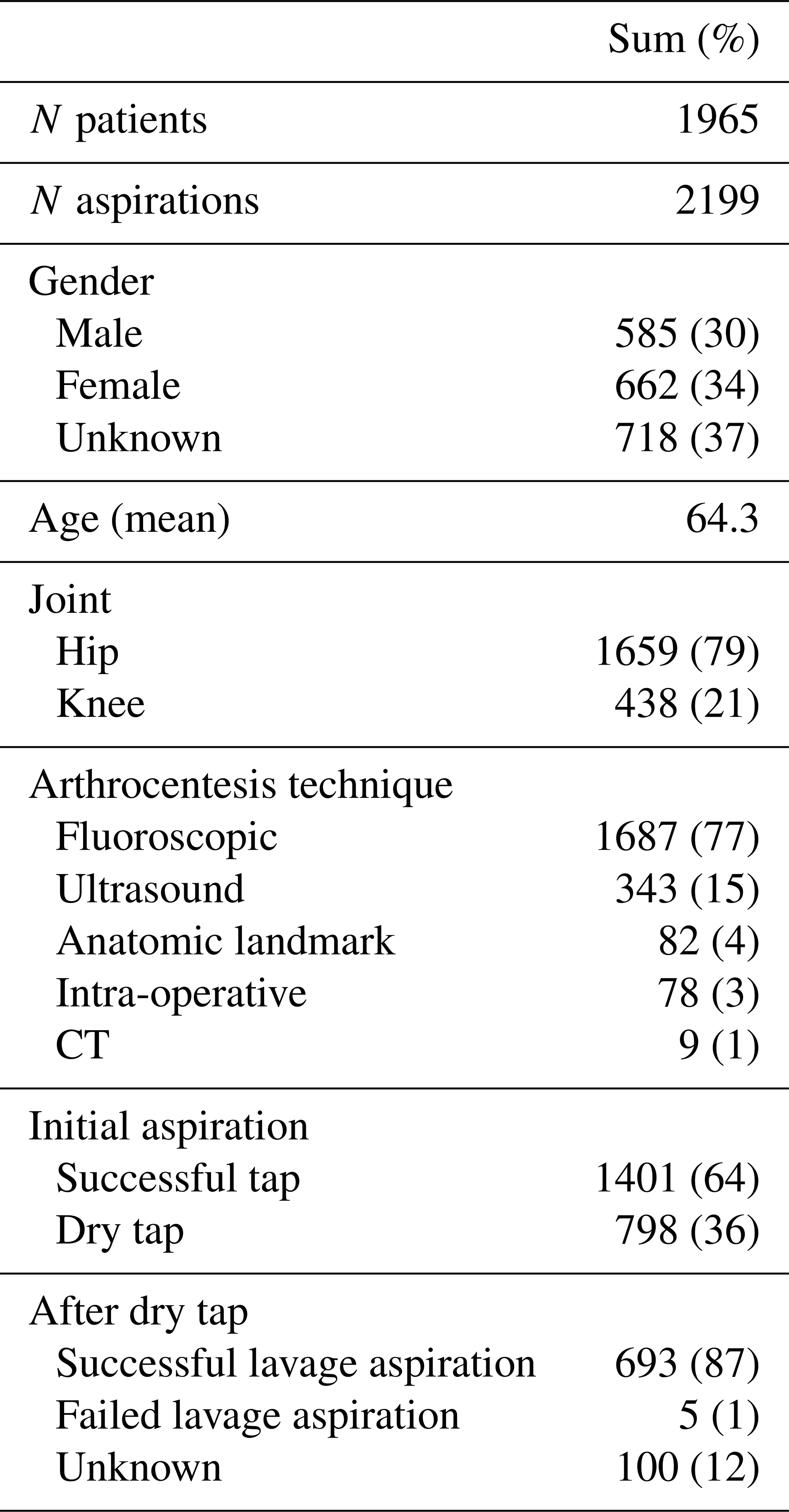
Across the 11 studies, 2199 aspirations were reported in 1965 patients. This discrepancy was due to repeat and/or bilateral aspirations in the same patient (Somme et al., 2003; Newman et al., 2017; Partridge et al., 2018) or failure to obtain synovial fluid despite lavage (Roberts et al., 1992; Somme et al., 2003). Of all aspirations, 1401 were successful and 798 resulted in a dry tap (Table 2). Patient demographics included 585 males and 662 females; sex was not reported for 718 patients (4 of 11 studies) (Roberts et al., 1992; Ali et al., 2006; Partridge et al., 2018; Barker et al., 2021). The mean patient age was 64.3 years (range 32–82). Across all studies, a total of 1659 unique hips and 438 unique knees were included. The higher number of aspirations reflects 102 repeat aspirations performed in hips. Most procedures were fluoroscopy guided (77 %), followed by ultrasound-guided aspiration (15 %). In seven studies, joint aspiration was performed in patients who demonstrated clinical manifestations and/or biochemical evidence indicative of PJI (Roberts et al., 1992; Ali et al., 2006; Newman et al., 2017; Li et al., 2019; Partridge et al., 2018; Barker et al., 2021; Christensen et al., 2022). The remaining four studies conducted aspirations as part of a routine pre-operative assessment prior to revision arthroplasty (Mulcahy et al., 1996; Somme et al., 2003; Heckmann et al., 2020; Treu et al., 2023).
3.4 Lavage aspiration technique
Considerable heterogeneity in terms of needle type and size, lavage volume, and arthrocentesis technique was noted (Table 1). Saline was the lavage fluid of choice in all included studies. Four studies specifically described the use of normal or isotonic saline (sodium chloride 0.9 %) in order to prevent cell lysis (Mulcahy et al., 1996; Li et al., 2019; Heckmann et al., 2020; Barker et al., 2021). Lavage aspiration of 10 mL saline was the most frequently reported volume (Roberts et al., 1992; Mulcahy et al., 1996; Ali et al., 2006; Li et al., 2019; Barker et al., 2021). Heckmann et al. (2020) described performing lavage aspiration intra-operatively prior to arthrotomy. Each joint was initially aspirated to remove the maximum possible amount of fluid, thereby simulating the clinical scenario of a dry tap. Subsequently, a lavage aspiration was conducted using 20 mL of sterile saline. Roberts et al. (1992) described often recovering only 2 to 3 mL after lavage of 10 mL saline; no other study reported the aspirated volume after lavage.
Spinal needles of 20G (gauge) were the most frequently reported needle type (Roberts et al., 1992; Ali et al., 2006; Li et al., 2019).
In over 82 % () of the studies, fluoroscopic-guided aspiration was the arthrocentesis technique of choice (Table 2). Ultrasound-guided aspiration was the second-most reported technique. The injection of contrast agents as lavage fluid was not performed in any of the included studies due to its bacteriostatic properties (Lopitaux et al., 1992; Glithero et al., 1993; Blake and Halasz, 1995; Taylor and Beggs, 1995; Cheung et al., 1997). However, the correct position of the needle within the joint was confirmed by an arthrogram in two studies (Mulcahy et al., 1996; Treu et al., 2023). Partridge et al. (2018) also described the injection of air to confirm the intra-articular position of the needle. Moreover, five studies reported that no attempt was made to infiltrate deeper than subcutaneous tissues with local anaesthetic because of concerns regarding bacteriostatic properties (Schmidt and Rosenkranz, 1970; Barrack and Harris, 1993; Kraemer et al., 1993; Roberts et al., 1992; Ali et al., 2006; Kung et al., 2012; Partridge et al., 2018; Li et al., 2019; Treu et al., 2023).
3.5 Primary outcome
Independent of arthrocentesis technique, the frequency of diagnosing PJI with lavage aspiration after dry tap was calculated to be 22 %. A total of 154 true positive PJIs were reported in 691 successful lavage aspirations after dry tap (Table 3).
Table 3Diagnostic characteristics of synovial fluid cultures after lavage aspiration.
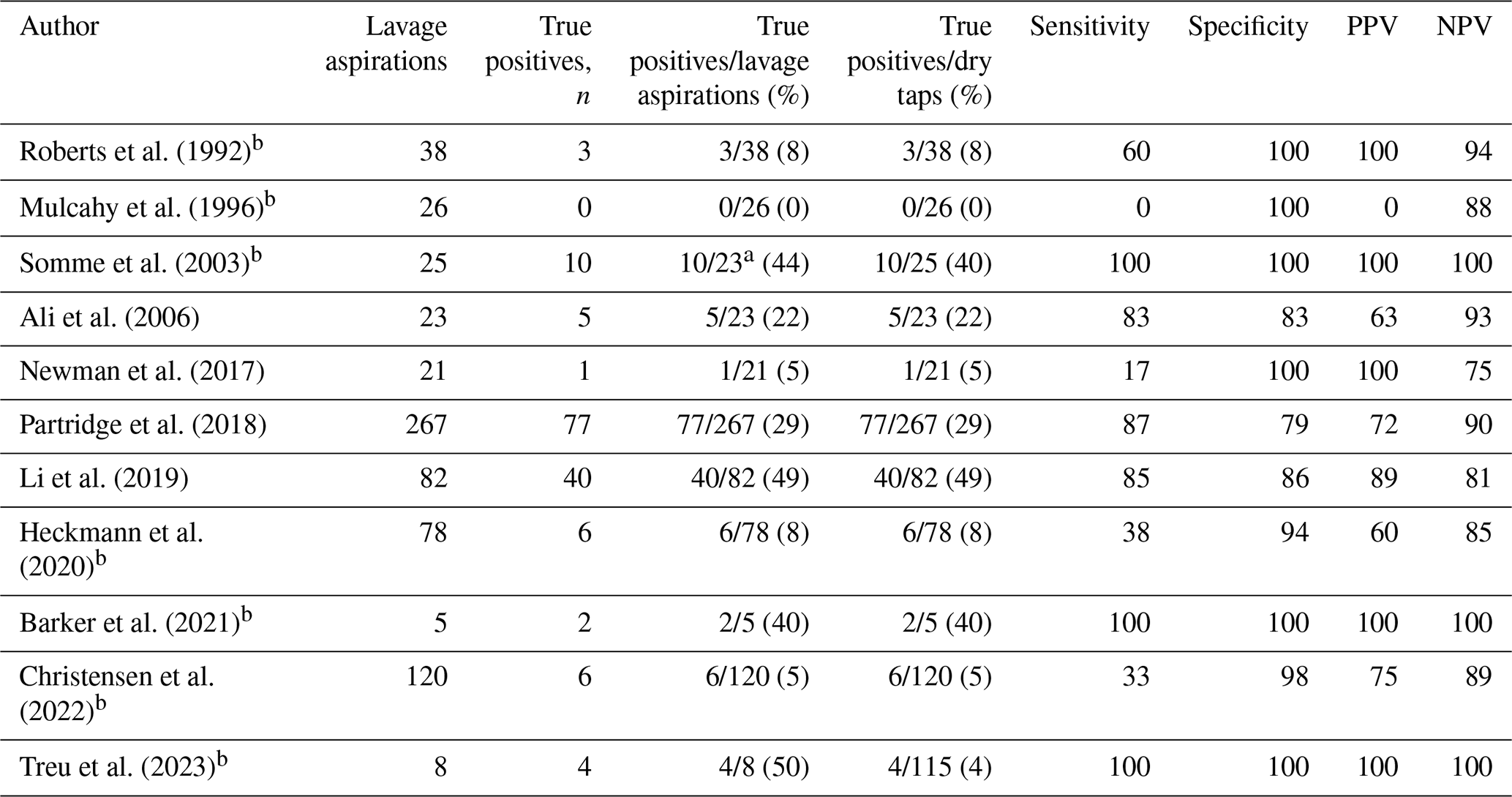
n – number of true positive aspirations after lavage; PPV – positive predictive value; NPV – negative predictive value; a 2 lavage aspirations failed; b (some) diagnostic characteristics calculated based on the reported data.
3.6 Diagnostic characteristics of lavage aspiration after dry tap
A total of 798 dry taps occurred in 2199 aspirations (36 %). In the majority of these (87 %), a successful lavage aspiration was performed (Table 2). In the remaining dry taps, a failed lavage aspiration (1 %) or unknown procedure (12 %) was reported.
3.6.1 Diagnostic characteristics of synovial fluid cultures after lavage aspiration
The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were described or calculated for the results of synovial fluid cultures after lavage aspiration in all included studies (Table 3).
The mean sensitivity was 66 % (range 0 %–100 %). Only Mulcahy et al. (1996) described a sensitivity of 0 % in 26 lavage aspirations, representing only 4 % of the lavage aspiration population. Three studies (Somme et al., 2003; Barker et al., 2021; Treu et al., 2023) reported a sensitivity of 100 % in a total of 36 lavage aspirations, which constituted 5 % of the lavage aspiration population.
The mean specificity was 89 % (range 79 %–100 %). Six studies (Roberts et al., 1992; Mulcahy et al., 1996; Somme et al., 2003; Partridge et al., 2018; Li et al., 2021; Barker et al., 2021) reported a specificity of 100 % in 121 lavage aspirations (18 %).
The mean PPV was 74 % (range 0 %–100 %). Mulcahy et al. (1996) described a PPV of 0 % in 26 lavage aspirations (4 %). Five studies (Roberts et al., 1992; Somme et al., 2003; Newman et al., 2017; Barker et al., 2021; Treu et al., 2023) reported a PPV of 100 % in 95 lavage aspirations (14 %).
The mean NPV was 89 % (range 75 %–100 %). Three studies (Somme et al., 2003; Barker et al., 2021; Treu et al., 2023) reported an NPV of 100 % in 36 lavage aspirations (5 %).
Across 691 successful lavage procedures, we identified 51 potential false-positive results based on a comparison with intra-operative cultures. This would correspond to a false-positive rate of approximately 7.4 %, which is reflected in the pooled specificity of 89 %. However, these data should be interpreted with utmost caution given the shortcomings of basing the diagnosis of low-grade PJI on just conventional culture results. For example, pre-operative analysis and culture of lavage synovial fluid could show a positive cytology (despite dilution), and the presence of Cutibacterium acnes and intra-operative cytology and histopathology could again be confirmatory for PJI, but tissue cultures could remain negative. This does not mean that the pre-operative culture result should be considered false-positive. To mitigate these risks, clinicians should always interpret (lavage) results in the context of broader diagnostic markers, as outlined in frameworks such as the EBJIS or MSIS.
It is furthermore important to acknowledge the considerable heterogeneity in culture systems and incubation protocols, when these were reported at all, which likely contributed to the wide variability observed across diagnostic performance metrics. Five studies employed blood culture media (Roberts et al., 1992; Ali et al., 2006; Partridge et al., 2018; Li et al., 2019; Barker et al., 2021), whereas Somme et al. (2003) utilised agar-based media. In the remaining studies, the culture system was not described.
3.6.2 Diagnostic characteristics of synovial fluid cytology after lavage aspiration
Heckmann et al. (2020) and Christensen et al. (2022) reported the diagnostic characteristics of WBC count >3000 cells µL−1 (Table 4). The mean sensitivity, specificity, PPV, and NPV were respectively 65 %, 89 %, 53 %, and 94 % in 198 lavage aspirations, representing 29 % of the lavage aspiration population.
The diagnostic characteristics of PMNs > 80 % were described by Newman et al. (2017), Heckmann et al. (2020) and Christensen et al. (2022). The mean sensitivity, specificity, PPV, and NPV were respectively 87 %, 81 %, 46 % and 96 % in 219 lavage aspirations, which constituted 32 % of the lavage aspiration population.
Table 4Diagnostic characteristics of secondary outcomes.
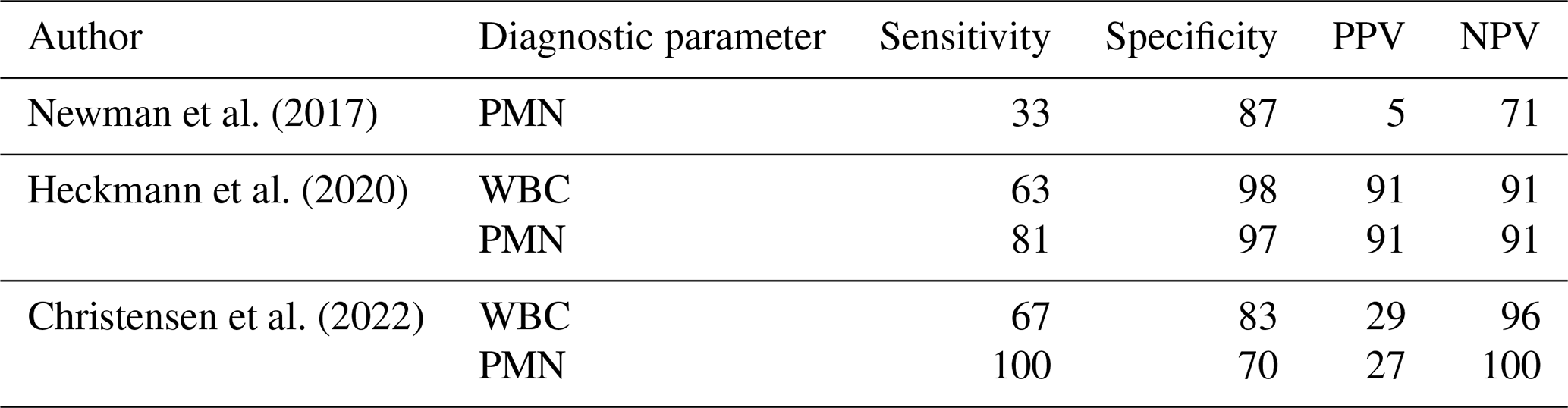
WBC – WBC count > 3000 cells µL−1; PMN – PMNs > 80 %; PPV – positive predictive value; NPV – negative predictive value.
3.7 Safety profile
Across all 11 included studies, no procedural complication attributable to this technique in comparison to successful taps was reported. The primary safety concerns identified in the literature are theoretical or indirect: the risk of introducing infection through the procedure, the generation of false-positive results through contamination during lavage, the dilution of synovial biomarkers leading to false-negative cell count interpretations, the bacteriostatic potential of injected substances, and the operator-dependent variability in success rates. These concerns are discussed with varying depth across studies, but none has been quantified through adverse event surveillance. The absence of a standardised approach to safety reporting across the included literature represents a notable gap.
This systematic review identified and critically appraised 11 studies evaluating the role of lavage aspiration after a dry tap in the diagnostic work-up of patients with potential PJI. The pooled incidence of dry tap was 36 %, consistent with previously reported rates of 30 %–45 % in the literature (Kung et al., 2012; Kanthawang et al., 2021; Ong et al., 2022; Treu et al., 2024). Among patients experiencing a dry tap, 154 PJIs were ultimately diagnosed, corresponding to an overall PJI prevalence of 19 % in this cohort. Notably, lavage aspiration yielded a correct PJI diagnosis in 22 % of cases in which aspiration after lavage was successful. These findings indicate that lavage aspiration might be a valuable adjunct when insufficient synovial fluid is obtained, and a dry tap should not – by any means – be considered exclusionary for PJI.
Several strategies have been proposed to reduce the occurrence of dry taps during diagnostic arthrocentesis. These include strict adherence to correct technique by an experienced clinician, the provision of adequate analgesia or sedation, and the use of image guidance (Heckmann et al., 2020; Serfaty et al., 2022; Treu et al., 2023, 2024). Ultrasound guidance, in particular, has been shown to decrease the frequency of dry aspirations by directly targeting effusions (Battaglia et al., 2011; Randelli et al., 2018; Treu et al., 2023). Moreover, multiple studies have reported superior diagnostic performance and enhanced safety profiles with ultrasound compared to fluoroscopic guidance (Battaglia et al., 2011; Randelli et al., 2018; Treu et al., 2023), suggesting that ultrasound may represent the preferred modality in this setting. Nevertheless, further investigations employing standardised arthrocentesis protocols are warranted to validate these findings and to determine whether such measures effectively reduce both dry taps and unexpected positive intra-operative cultures (UPICs).
If a dry tap occurs despite the measures described above, several options remain for confirming or excluding a PJI. In addition to lavage aspiration, these include repeat aspiration after an interval, open biopsy, and intra-operative tests – such as frozen sections and alpha-defensin – performed during revision arthroplasty (Sigmund et al., 2019; Russo et al., 2025; Sigmund et al., 2025). Image-guided synovial biopsy appears to be a particularly promising option, as it could be done directly when a dry tap is encountered, has high diagnostic yield, and allows for both microbiological as well as histopathological analysis (Macnair et al., 2023). However, it does not provide a PMN %, which remains one of the most valuable pre-operative diagnostic criteria for PJI. An RCT comparing saline lavage aspiration with synovial biopsy in the setting of a dry tap would therefore be of considerable interest. When interpreting results from lavage aspiration, several considerations should be made. First, culture sensitivity after lavage aspiration averaged 66 %, consistent with the wide variability (12 %–100 %) reported for standard aspiration (Fitzgerald et al., 1977; O'Neill and Harris, 1984; Magnuson et al., 1988; Levitsky et al., 1991; Barrack and Harris, 1993; Kraemer et al., 1993; Lachiewicz et al., 1996; Spangehl et al., 1999). Specificity averaged 89 %, also consistent with the 81 %–100 % range reported for standard aspiration (Magnuson et al., 1988; Levitsky et al., 1991; Barrack and Harris, 1993; Kraemer et al., 1993; Tigges et al., 1993; Duff et al., 1996; Fehring and Cohen, 1996; Lachiewicz et al., 1996; Spangehl et al., 1999; Teller et al., 2000). Second, saline lavage dilutes synovial fluid, lowering absolute WBC counts but preserving relative PMN percentages (Heckmann et al., 2020; Christensen et al., 2022). Thus, the threshold of PMNs > 80 % remains a reliable marker, while absolute WBC counts must be interpreted with caution. If – after dilution – the fluid sample still contains over 1500–3000 white blood cells (WBCs) per microlitre, this of course remains a strong argument for the existence of PJI.
None of the studies included reported safety concerns with lavage aspiration. Nevertheless, the potential introduction of pathogens into the joint and the risk of false-positive results remain concerns that are not fully mitigated by the available evidence. This small risk must be balanced against the benefit of avoiding a missed diagnosis, as approximately one in five PJIs were identified only after lavage aspiration.
This review has several limitations. All included studies were level IV case series, most with retrospective designs, small sample sizes, and potential selection bias. Considerable heterogeneity in lavage technique and outcome reporting further limits the generalisability of findings. Moreover, no standardised definition of PJI was uniformly applied across the studies; therefore, the diagnostic criteria reported by each study were accepted as originally defined by the respective authors. Finally, the lack of a standardised culture platform or incubation protocol likely contributed to the marked variability in reported sensitivity and specificity among the studies.
Approximately one in three aspirations result in a dry tap. Saline lavage aspiration provides analysable fluid in nearly all cases and appears to enable the diagnosis of PJI in roughly one out of five patients in whom standard aspiration fails. However, more robust evidence is needed before it can be recommended as a universal technique.
The data used to support the findings of this study are included in the article (Sect. 3, and Tables 2, 3, and 4).
SB and GV were responsible for the conceptualisation and design of the systematic review. SB drafted the work. SB and GV analysed and interpreted the data. SG, MD, AS, and WJM revised and critically appraised the article. All authors approved the final version of the article and agreed to be accountable for all aspects of the work. All authors fulfil the criteria for authorship by ICMJE.
At least one of the (co-)authors is a member of the editorial board of Journal of Bone and Joint Infection. The peer-review process was guided by an independent editor, and the authors also have no other competing interests to declare.
This systematic review does not constitute original human or animal research and therefore did not require formal ethics committee approval or informed consent from participants.
Publisher's note: Copernicus Publications remains neutral with regard to jurisdictional claims made in the text, published maps, institutional affiliations, or any other geographical representation in this paper. The authors bear the ultimate responsibility for providing appropriate place names. Views expressed in the text are those of the authors and do not necessarily reflect the views of the publisher.
This paper was edited by Marta Sabater-Martos and reviewed by two anonymous referees.
Ali, F., Wilkinson, J. M., Cooper, J. R., Kerry, R. M., Hamer, A. J., Norman, P., and Stockley, I.: Accuracy of joint aspiration for the preoperative diagnosis of infection in total hip arthroplasty, J. Arthroplasty, 21, 221–226, https://doi.org/10.1016/j.arth.2005.05.027, 2006.
Barker, C. J., Marriot, A., Khan, M., Oswald, T., Tingle, S. J., Partington, P. F., Carluke, I., and Reed, M. R.: Hip aspiration culture: analysing data from a single operator series investigating periprosthetic joint infection, J. Bone Joint Infect., 6, 165–170, https://doi.org/10.5194/jbji-6-165-2021, 2021.
Barrack, R. L. and Harris, W. H.: The value of aspiration of the hip joint before revision total hip arthroplasty, J. Bone Joint Surg. Am., 75, 66–76, https://doi.org/10.2106/00004623-199301000-00010, 1993.
Battaglia, M., Vannini, F., Guaraldi, F., Rossi, G., Biondi, F., and Sudanese, A.: Validity of preoperative ultrasound-guided aspiration in the revision of hip prosthesis, Ultrasound Med. Biol., 37, 1977–1983, https://doi.org/10.1016/j.ultrasmedbio.2011.09.004, 2011.
Blake, M. P. and Halasz, S. J.: The effects of X-ray contrast media on bacterial growth, Australas. Radiol., 39, 10–13, https://doi.org/10.1111/j.1440-1673.1995.tb00223.x, 1995.
Burgo, F., Stangl, W. P., Lumban Gaol, I., Kvederas, G., Reed, M., Gado, I., Al Maskari, S., Olivetto, R., and Davies, A.: HK21: Should saline be injected into a joint during a dry aspiration (tap)? ICMORTHO, https://www.icmortho.org/_files/ugd/34d74b_8cced98f92f241f98b2afb4e71d6e1d3.pdf, last access: 30 October 2025.
Cheung, A., Lachiewicz, P. F., and Renner, J. B.: The role of aspiration and contrast-enhanced arthrography in evaluating the uncemented hip arthroplasty, AJR Am. J. Roentgenol., 168, 1305–1309, https://doi.org/10.2214/ajr.168.5.9129431, 1997.
Christensen, T. H., Ong, J., Lin, D., Aggarwal, V. K., Schwarzkopf, R., and Rozell, J. C.: How does a “dry tap” impact the accuracy of preoperative aspiration results in predicting chronic periprosthetic joint infection?, J. Arthroplasty, 37, 925–929, https://doi.org/10.1016/j.arth.2022.01.066, 2022.
Duff, G. P., Lachiewicz, P. F., and Kelley, S. S.: Aspiration of the knee joint before revision arthroplasty, Clin. Orthop. Relat. R., 331, 132–139, https://doi.org/10.1097/00003086-199610000-00018, 1996.
Durst, C. R., Rezzadeh, K. T., Than, J. P., Rajaee, S. S., and Spitzer, A. I.: Intra-Articular Corticosteroid Injections Into a Preexisting Total Knee Arthroplasty are Associated With Increased Risk of Periprosthetic Joint Infection and Revision, Arthroplasty Today, 24, 101237, https://doi.org/10.1016/j.artd.2023.101237, 2023.
Fehring, T. K. and Cohen, B.: Aspiration as a guide to sepsis in revision total hip arthroplasty, J. Arthroplasty, 11, 543–547, https://doi.org/10.1016/S0883-5403(96)80107-0, 1996.
Fitzgerald Jr., R. H., Nolan, D. R., Ilstrup, D. M., Van Scoy, R. E., Washington 2nd, J. A., and Coventry, M. B.: Deep wound sepsis following total hip arthroplasty, J. Bone Joint Surg. Am., 59, 847–855, 1977.
Geirsson, A. J., Statkevicius, S., and Vikingsson, A.: Septic arthritis in Iceland 1990–2002: increasing incidence due to iatrogenic infections, Ann. Rheum. Dis., 67, 638–643, https://doi.org/10.1136/ard.2007.077131, 2008.
Glithero, P. R., Grigoris, P., Harding, L. K., Hesslewood, S. R., and McMinn, D. J.: White cell scans and infected joint replacements: failure to detect chronic infection, J. Bone Joint Surg. Br., 75, 371–374, https://doi.org/10.1302/0301-620X.75B3.8496202, 1993.
Heckmann, N. D., Nahhas, C. R., Yang, J., Della Valle, C. J., Yi, P. H., Culvern, C. N., and Klein, G. R.: Saline lavage after a “dry tap”, Bone Joint J., 102-B, 138–144, https://doi.org/10.1302/0301-620X.102B6.BJJ-2019-1679.R1, 2020.
Kanthawang, T., Bodden, J., Joseph, G. B., Vail, T., Ward, D., Patel, R., and Link, T. M.: Diagnostic value of fluoroscopy-guided hip aspiration for periprosthetic joint infection, Skeletal Radiol., 50, 2245–2254, https://doi.org/10.1007/s00256-021-03795-8, 2021.
Keating, T. C., Guntin, J., Harkin, W. E., Weintraub, M. T., Karas, V., and Berger, R. A.: Low risk of acute iatrogenic periprosthetic joint infection after prosthetic joint aspiration, J. Arthroplasty, 38, 1861–1863, https://doi.org/10.1016/j.arth.2023.03.053, 2023.
Kraemer, W. J., Saplys, R., Waddell, J. P., and Morton, J.: Bone scan, gallium scan, and hip aspiration in the diagnosis of infected total hip arthroplasty, J. Arthroplasty, 8, 611–616, https://doi.org/10.1016/0883-5403(93)90008-R, 1993.
Kung, J. W., Yablon, C., Huang, E. S., Hennessey, H., and Wu, J. S.: Clinical and radiologic predictive factors of septic hip arthritis, AJR Am. J. Roentgenol., 199, 868–872, https://doi.org/10.2214/AJR.10.6273, 2012.
Lachiewicz, P. F., Rogers, G. D., and Thomason, H. C.: Aspiration of the hip joint before revision total hip arthroplasty: clinical and laboratory factors influencing attainment of a positive culture, J. Bone Joint Surg. Am., 78, 749–754, https://doi.org/10.2106/00004623-199605000-00015, 1996.
Levitsky, K. A., Hozack, W. J., Balderston, R. A., Rothman, R. H., Gluckman, S. J., Maslack, M. M., and Booth Jr., R. E.: Evaluation of the painful prosthetic joint: relative value of bone scan, sedimentation rate, and joint aspiration, J. Arthroplasty, 6, 237–244, https://doi.org/10.1016/S0883-5403(06)80170-1, 1991.
Li, R., Lu, Q., Chai, W., Hao, L. B., Lu, S. B., and Chen, J. Y.: Saline solution lavage and reaspiration for culture with a blood culture system is a feasible method for diagnosing periprosthetic joint infection in patients with insufficient synovial fluid, J. Bone Joint Surg. Am., 101, 1004–1009, https://doi.org/10.2106/JBJS.18.01052, 2019.
Li, R., Li, X., Ni, M., Zheng, Q. Y., Zhang, G. Q., and Chen, J. Y.: Anatomic landmark-guided hip aspiration in the diagnosis of periprosthetic joint infection, Orthopedics, 44, e85–e90, https://doi.org/10.3928/01477447-20201007-04, 2021.
Lopitaux, R., Levai, J. P., Raux, P., Hermet, R., Grenier-Gaudin, A., and Sirot, J.: Intérêt de la ponction-arthrographie de hanche dans le diagnostic d'infection sur prothèse totale, Rev. Chir. Orthop. Reparatrice Appar. Mot., 78, 34–37, 1992.
Macnair, R., Rajakulasingam, R., Singh, S., Khoo, M., Upadhyay, B., Hargunani, R., and Pressney, I.: Image-guided synovial biopsy with a focus on infection, Skeletal Radiol., 52, 831–841, https://doi.org/10.1007/s00256-022-04245-9, 2023.
Magnuson, J. E., Brown, M. L., Hauser, M. F., Berquist, T. H., Fitzgerald Jr., R. H., and Klee, G. G.: In-111-labeled leukocyte scintigraphy in suspected orthopedic prosthesis infection: comparison with other imaging modalities, Radiology, 168, 235–239, https://doi.org/10.1148/radiology.168.1.3380966, 1988.
McNally, M., Sousa, R., Wouthuyzen-Bakker, M., Chen, A. F., Soriano, A., Vogely, H. C., Gumaste, V., and Alt, V.: The EBJIS definition of periprosthetic joint infection, Bone Joint J., 103-B, 18–25, https://doi.org/10.1302/0301-620X.103B1.BJJ-2020-1381.R1, 2021.
Mills, E. S., Elman, M. B., and Foran, J. R. H.: The Risk of Acute Infection Following Intra-articular Corticosteroid Injection Into a Pre-existing Total Knee Arthroplasty, J. Arthroplasty, 33, 216–219, https://doi.org/10.1016/j.arth.2017.07.029, 2018.
Mulcahy, D. M., Fenelon, G. C., and McInerney, D. P.: Aspiration arthrography of the hip joint: its uses and limitations in revision hip surgery, J. Arthroplasty, 11, 64–68, https://doi.org/10.1016/S0883-5403(96)80162-8, 1996.
Newman, J. M., George, J., Klika, A. K., Hatem, S. F., Barsoum, W. K., North, W. T., and Higuera, C. A.: What is the diagnostic accuracy of aspirations performed on hips with antibiotic cement spacers?, Clin. Orthop. Relat. Res., 475, 204–211, https://doi.org/10.1007/s11999-016-5093-8, 2017.
O'Neill, D. A. and Harris, W. H.: Failed total hip replacement: assessment by plain radiographs, arthrograms, and aspiration of the hip joint, J. Bone Joint Surg. Am., 66, 540–546, 1984.
Ong, J., Tang, A., Rozell, J. C., Babb, J. S., Schwarzkopf, R., and Lin, D.: Factors predicting hip joint aspiration yield or “dry taps” in patients with total hip arthroplasty, J. Orthop. Surg. Res., 17, 42, https://doi.org/10.1186/s13018-022-02942-8, 2022.
Partridge, D. G., Winnard, C., Townsend, R., Cooper, R., and Stockley, I.: Joint aspiration, including culture of reaspirated saline after a “dry tap”, is sensitive and specific for the diagnosis of hip and knee prosthetic joint infection, Bone Joint J., 100-B, 749–754, https://doi.org/10.1302/0301-620X.100B6.BJJ-2017-0970.R2, 2018.
Petersen, S. K., Knudsen, A., and Varnum, C.: Low frequency of septic arthritis after arthrocentesis and intra-articular glucocorticoid injection, Scand. J. Rheumatol., 48, 321–324, https://doi.org/10.1080/03009742.2018.1538159, 2019.
Rajakulasingam, R., Cleaver, L., Khoo, M., Pressney, I., Upadhyay, B., and Palanivel, S.: Introducing image-guided synovial aspiration and biopsy in assessing peri-prosthetic joint infection: an early single-centre experience, Skeletal Radiol., 50, 2031–2040, https://doi.org/10.1007/s00256-021-03774-z, 2021.
Randelli, F., Brioschi, M., Randelli, P., Ambrogi, F., Sdao, S., and Aliprandi, A.: Fluoroscopy- vs ultrasound-guided aspiration techniques in the management of periprosthetic joint infection: which is the best?, Radiol. Med., 123, 28–35, https://doi.org/10.1007/s11547-017-0811-1, 2018.
Roberts, P., Walters, A. J., and McMinn, D. J.: Diagnosing infection in hip replacements: the use of fine-needle aspiration and radiometric culture, J. Bone Joint Surg. Br., 74, 265–269, https://doi.org/10.1302/0301-620X.74B2.1544966, 1992.
Rodriguez, H. C., Mekkawy, K. L., Watkins, A., Roche, M. W., Burke, W. V., and Gosthe, R. G.: Risk of Periprosthetic Joint Infection After Intra-Articular Corticosteroid Injection Following Unicompartmental Knee Arthroplasty, J. Arthroplasty, 38, 815–819, https://doi.org/10.1016/j.arth.2022.12.005, 2023.
Roecker, Z., Quinlan, N. D., Browne, J. A., and Werner, B. C.: Risk of Periprosthetic Infection Following Intra-Articular Corticosteroid Injections After Total Knee Arthroplasty, J. Arthroplasty, 35, 1090–1094, https://doi.org/10.1016/j.arth.2019.11.017, 2020.
Russo, A., Budin, M., Luo, T. D., Uribe, A. C., Gehrke, T., and Citak, M.: Open biopsy is a safe procedure in patients who have suspected periprosthetic joint infection of the hip or knee and double-negative joint aspiration, J. Arthroplasty, 40, 3265–3270, https://doi.org/10.1016/j.arth.2025.05.102, 2025.
Schmidt, R. M. and Rosenkranz, H. S.: Antimicrobial activity of local anesthetics: lidocaine and procaine, J. Infect. Dis., 121, 597–607, https://doi.org/10.1093/infdis/121.6.597, 1970.
Serfaty, A., Jacobs, A., Gyftopoulos, S., and Samim, M.: Likelihood of hip infection with image-guided hip aspiration dry tap: a 10-year retrospective study, Skeletal Radiol., 51, 1947–1958, https://doi.org/10.1007/s00256-022-04046-0, 2022.
Sigmund, I. K., Holinka, J., Lang, S., Stenicka, S., Staats, K., Hobusch, G., Lass, R., Windhager, R., and Presterl, E.: A comparative study of intraoperative frozen section and alpha defensin lateral flow test in the diagnosis of periprosthetic joint infection, Acta Orthop., 90, 105–110, https://doi.org/10.1080/17453674.2019.1567153, 2019.
Sigmund, I. K., Bue, M., Kruse Jensen, L., McNally, M. A., Parvizi, J., Sabater-Martos, M., and ICM Meeting 2025: Histological analysis in the diagnosis of periprosthetic joint infection of the hip and knee: a systematic review and meta-analysis, Bone Joint J., 107-B, 1158–1164, https://doi.org/10.1302/0301-620X.107B11.BJJ-2025-0289.R1, 2025.
Somme, D., Ziza, J. M., Desplaces, N., Chicheportiche, V., Chazerain, P., Leonard, P., and Pouchot, J.: Contribution of routine joint aspiration to the diagnosis of infection before hip revision surgery, Joint Bone Spine, 70, 489–495, https://doi.org/10.1016/S1297-319X(03)00058-7, 2003.
Spangehl, M. J., Masri, B. A., O'Connell, J. X., and Duncan, C. P.: Prospective analysis of preoperative and intraoperative investigations for the diagnosis of infection at the sites of two hundred and two revision total hip arthroplasties, J. Bone Joint Surg. Am., 81, 672–683, https://doi.org/10.2106/00004623-199905000-00008, 1999.
Taylor, T. and Beggs, I.: Fine needle aspiration in infected hip replacements, Clin. Radiol., 50, 149–152, https://doi.org/10.1016/S0009-9260(05)83044-2, 1995.
Teller, R. E., Christie, M. J., Martin, W., Nance, E. P., and Haas, D. W.: Sequential indium-labeled leukocyte and bone scans to diagnose prosthetic joint infection, Clin. Orthop. Relat. Res., 373, 241–247, https://doi.org/10.1097/00003086-200004000-00029, 2000.
Tigges, S., Stiles, R. G., Meli, R. J., and Roberson, J. R.: Hip aspiration: a cost-effective and accurate method of evaluating the potentially infected hip prosthesis, Radiology, 189, 485–488, https://doi.org/10.1148/radiology.189.2.8210377, 1993.
Treu, E. A., Cushman, D. M., Wheelwright, J. C., Blackburn, B. E., Teramoto, M., and Archibeck, M. J.: Is ultrasound-guided hip aspiration more successful than fluoroscopic-guided aspiration in diagnosing prosthetic joint infection?, J. Bone Joint Infect., 8, 151–163, https://doi.org/10.5194/jbji-8-151-2023, 2023.
Treu, E. A., Behrens, N. F., Blackburn, B. E., Cushman, D. M., and Archibeck, M. J.: A “dry tap” in prosthetic joint infection workup of total hip arthroplasty is not reassuring, J. Arthroplasty, 39, S220–S224, https://doi.org/10.1016/j.arth.2024.02.029, 2024.
Zimmerli, W., Waldvogel, F. A., Vaudaux, P., and Nydegger, U. E.: Pathogenesis of foreign body infection: description and characteristics of an animal model, J. Infect. Dis., 146, 487–497, https://doi.org/10.1093/infdis/146.4.487, 1982.
When infection around an artificial hip or knee is suspected, joint fluid sampling is essential but often unsuccessful. We performed a systematic review to evaluate whether rinsing the joint with sterile salt water after an unsuccessful attempt improves diagnosis. Our findings show that this approach is safe, yields testable fluid in nearly all cases, and identifies infection in about one in five patients that would otherwise be missed.
When infection around an artificial hip or knee is suspected, joint fluid sampling is...